

Impaired haemophilus influenzae type b transplacental antibody transmission and declining antibody avidity through the first year of life represent potential vulnerabilities for HIV-exposed but -uninfected infants
- PMID: 25298109
- PMCID: PMC4248779
- DOI: 10.1128/CVI.00356-14
Impaired haemophilus influenzae type b transplacental antibody transmission and declining antibody avidity through the first year of life represent potential vulnerabilities for HIV-exposed but -uninfected infants
Abstract
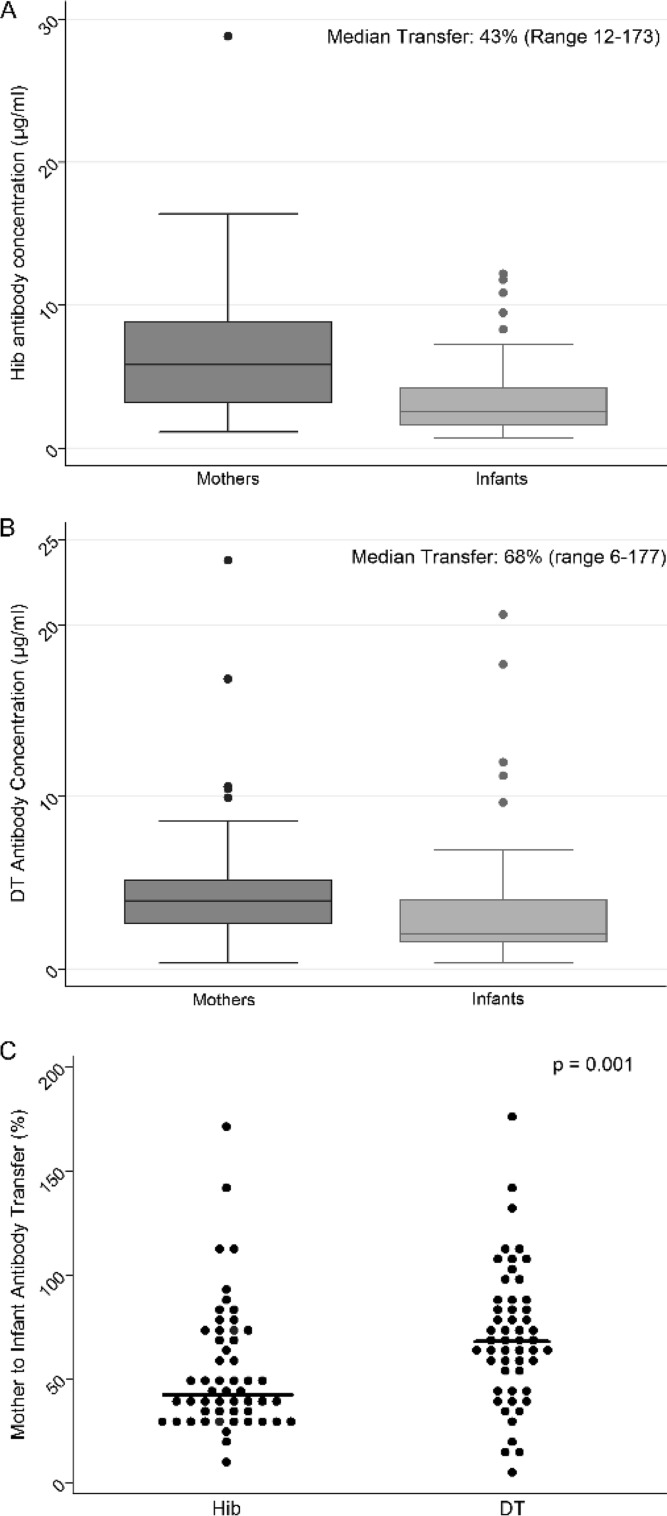
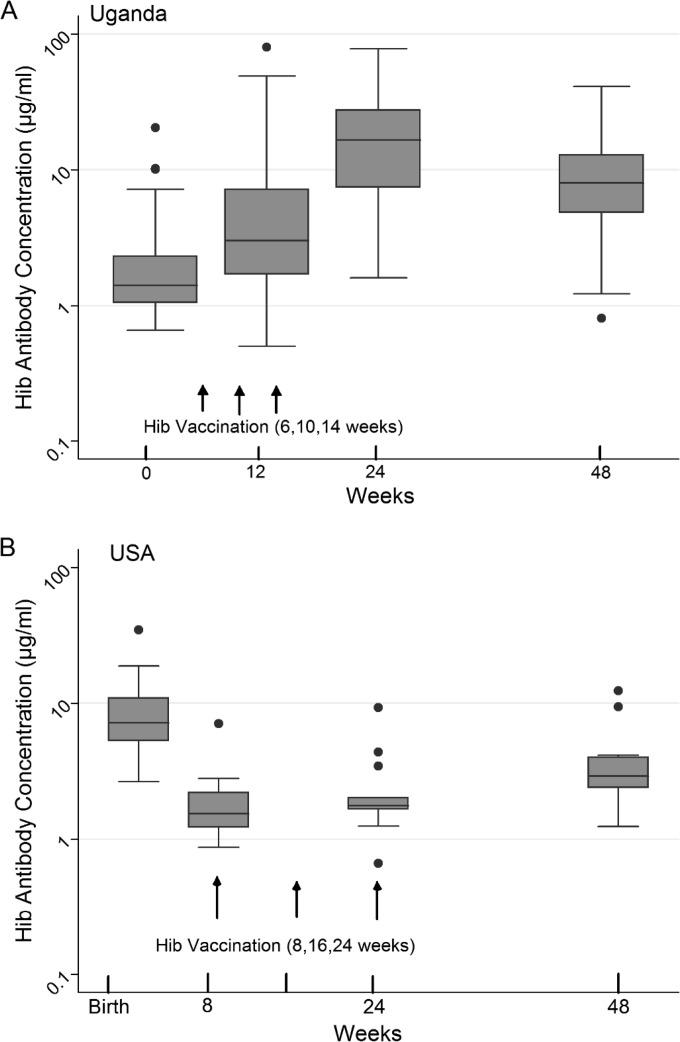
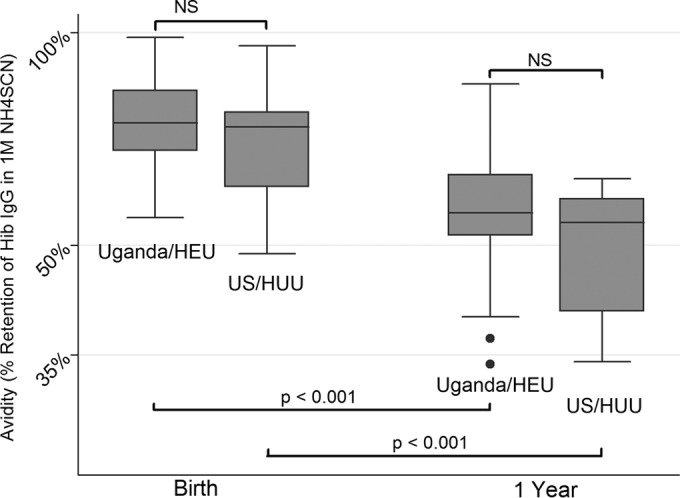
To determine whether immune function is impaired among HIV-exposed but -uninfected (HEU) infants born to HIV-infected mothers and to identify potential vulnerabilities to vaccine-preventable infection, we characterized the mother-to-infant placental transfer of Haemophilus influenzae type b-specific IgG (Hib-IgG) and its levels and avidity after vaccination in Ugandan HEU infants and in HIV-unexposed U.S. infants. Hib-IgG was measured by enzyme-linked immunosorbent assay in 57 Ugandan HIV-infected mothers prenatally and in their vaccinated HEU infants and 14 HIV-unexposed U.S. infants at birth and 12, 24, and 48 weeks of age. Antibody avidity at birth and 48 weeks of age was determined with 1 M ammonium thiocyanate. A median of 43% of maternal Hib-IgG was transferred to HEU infants. Although its level was lower in HEU infants than in U.S. infants at birth (P < 0.001), Hib-IgG was present at protective levels (>1.0 μg/ml) at birth in 90% of HEU infants and all U.S. infants. HEU infants had robust Hib-IgG responses to a primary vaccination. Although Hib-IgG levels declined from 24 to 48 weeks of age in HEU infants, they were higher than those in U.S. infants (P = 0.002). Antibody avidity, comparable at birth, declined by 48 weeks of age in both populations. Early vaccination of HEU infants may limit an initial vulnerability to Hib disease resulting from impaired transplacental antibody transfer. While initial Hib vaccine responses appeared adequate, the confluence of lower antibody avidity and declining Hib-IgG levels in HEU infants by 12 months support Hib booster vaccination at 1 year. Potential immunologic impairments of HEU infants should be considered in the development of vaccine platforms for populations with high maternal HIV prevalence.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures

Similar articles
-
Safety and antibody persistence following Haemophilus influenzae type b conjugate or pneumococcal polysaccharide vaccines given before pregnancy in women of childbearing age and their infants.Pediatr Infect Dis J. 2001 Oct;20(10):931-40. doi: 10.1097/00006454-200110000-00005. Pediatr Infect Dis J. 2001. PMID: 11642626 Clinical Trial.
-
Antibody responses to vaccination among South African HIV-exposed and unexposed uninfected infants during the first 2 years of life.Clin Vaccine Immunol. 2013 Jan;20(1):33-8. doi: 10.1128/CVI.00557-12. Epub 2012 Oct 31. Clin Vaccine Immunol. 2013. PMID: 23114697 Free PMC article.
-
Maternal HIV infection and antibody responses against vaccine-preventable diseases in uninfected infants.JAMA. 2011 Feb 9;305(6):576-84. doi: 10.1001/jama.2011.100. JAMA. 2011. PMID: 21304083
-
Maternal immunization with Haemophilus influenzae type b vaccines in different populations.Vaccine. 2003 Jul 28;21(24):3455-9. doi: 10.1016/s0264-410x(03)00350-5. Vaccine. 2003. PMID: 12850359 Review.
-
Circulating innate and adaptive immunity against anti-Haemophilus influenzae type b.Hum Antibodies. 2019;27(3):201-212. doi: 10.3233/HAB-190373. Hum Antibodies. 2019. PMID: 30958343 Review.
Cited by
-
Transfer of Maternal Antimicrobial Immunity to HIV-Exposed Uninfected Newborns.Front Immunol. 2016 Aug 31;7:338. doi: 10.3389/fimmu.2016.00338. eCollection 2016. Front Immunol. 2016. PMID: 27630640 Free PMC article. Review.
-
Deficit of IgG2 in HIV-positive pregnant women is responsible of inadequate IgG2 levels in their HIV-uninfected children in Malawi.Med Microbiol Immunol. 2018 Aug;207(3-4):175-182. doi: 10.1007/s00430-018-0537-2. Epub 2018 Feb 27. Med Microbiol Immunol. 2018. PMID: 29488063
-
Effects of Maternal HIV Infection on Early Kaposi Sarcoma-Associated Herpesvirus Seroconversion in a Kenyan Mother-Infant Cohort.J Infect Dis. 2023 Nov 11;228(10):1357-1366. doi: 10.1093/infdis/jiad310. J Infect Dis. 2023. PMID: 37536370 Free PMC article.
-
Placental Transfer of Respiratory Syncytial Virus Antibody Among HIV-Exposed, Uninfected Infants.J Pediatric Infect Dis Soc. 2020 Jul 13;9(3):349-356. doi: 10.1093/jpids/piz056. J Pediatric Infect Dis Soc. 2020. PMID: 31549157 Free PMC article.
-
HIV-Exposed Uninfected Infants Show Robust Memory B-Cell Responses in Spite of a Delayed Accumulation of Memory B Cells: an Observational Study in the First 2 Years of Life.Clin Vaccine Immunol. 2016 Jul 5;23(7):576-85. doi: 10.1128/CVI.00149-16. Print 2016 Jul. Clin Vaccine Immunol. 2016. PMID: 27170641 Free PMC article.
References
-
- St. Geme J. 2008. Haemophilus influenzae, p 892–897 In Long S, Pickering L, Prober C. (ed), Principles and practice of pediatric infectious diseases, 3rd ed. Elsevier, Inc., Philadelphia, PA.
-
- Peltola H. 2000. Worldwide Haemophilus influenzae type b disease at the beginning of the 21st century: global analysis of the disease burden 25 years after the use of the polysaccharide vaccine and a decade after the advent of conjugates. Clin. Microbiol. Rev. 13:302–317. 10.1128/CMR.13.2.302-317.2000. - DOI - PMC - PubMed
-
- Watt JP, Wolfson LJ, O'Brien KL, Henkle E, Deloria-Knoll M, McCall N, Lee E, Levine OS, Hajjeh R, Mulholland K, Cherian T. 2009. Burden of disease caused by Haemophilus influenzae type b in children younger than 5 years: global estimates. Lancet 374:903–911. 10.1016/S0140-6736(09)61203-4. - DOI - PubMed
-
- von Gottberg A, Cohen C, Whitelaw A, Chhagan M, Flannery B, Cohen AL, de Gouveia L, Plessis MD, Madhi SA, Klugman KP, Group for Enteric, Respiratory, Meningeal Disease Surveillance in South Africa (GERMS-SA) 2012. Invasive disease due to Haemophilus influenzae serotype b ten years after routine vaccination, South Africa, 2003-2009. Vaccine 30:565–571. 10.1016/j.vaccine.2011.11.066. - DOI - PubMed
-
- Lee EH, Lewis RF, Makumbi I, Kekitiinwa A, Ediamu TD, Bazibu M, Braka F, Flannery B, Zuber PL, Feikin DR. 2008. Haemophilus influenzae type b conjugate vaccine is highly effective in the Ugandan routine immunization program: a case-control study. Trop. Med. Int. Health 13:495–502. 10.1111/j.1365-3156.2008.02027.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
