

Comparison of trends in sepsis incidence and coding using administrative claims versus objective clinical data
- PMID: 25258352
- PMCID: PMC4318944
- DOI: 10.1093/cid/ciu750
Comparison of trends in sepsis incidence and coding using administrative claims versus objective clinical data
Abstract
Background: National reports of a dramatic rise in sepsis incidence are largely based on analyses of administrative databases. It is unclear if these estimates are biased by changes in coding practices over time.
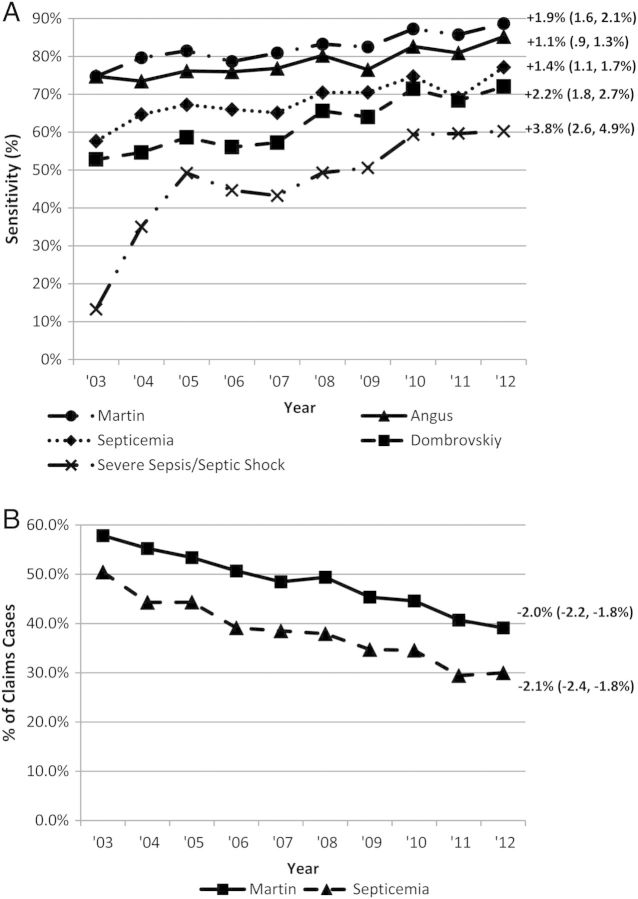
Methods: We calculated linear trends in the annual incidence of septicemia, sepsis, and severe sepsis at 2 academic hospitals from 2003 to 2012 using 5 different claims methods and compared case identification rates to selected objective clinical markers, including positive blood cultures, vasopressors, and/or lactic acid levels.
Results: The annual incidence of hospitalizations with sepsis claims increased over the decade, ranging from a 54% increase for the method combining septicemia, bacteremia, and fungemia codes (P < .001 for linear trend) to a 706% increase for explicit severe sepsis/septic shock codes (P = .001). In contrast, the incidence of hospitalizations with positive blood cultures decreased by 17% (P = .006), and hospitalizations with positive blood cultures with concurrent vasopressors and/or lactic acidosis remained stable (P = .098). The sensitivity of sepsis claims for capturing hospitalizations with positive blood cultures with concurrent vasopressors and/or lactic acidosis increased (P < .001 for all methods), whereas the proportion of septicemia hospitalizations with positive blood cultures decreased from 50% to 30% (P < .001).
Conclusions: The incidence of hospitalizations with sepsis codes rose dramatically while hospitalizations with corresponding objective clinical markers remained stable or decreased. Coding for sepsis has become more inclusive, and septicemia diagnoses are increasingly being applied to patients without positive blood cultures. These changes likely explain some of the apparent rise in sepsis incidence and underscore the need for more reliable surveillance methods.
Keywords: administrative coding; bloodstream infections; incidence; sepsis; septicemia.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures

Similar articles
-
Trends in sepsis and infection sources in the United States. A population-based study.Ann Am Thorac Soc. 2015 Feb;12(2):216-20. doi: 10.1513/AnnalsATS.201411-498BC. Ann Am Thorac Soc. 2015. PMID: 25569845 Free PMC article.
-
Improving documentation and coding for acute organ dysfunction biases estimates of changing sepsis severity and burden: a retrospective study.Crit Care. 2015 Sep 14;19(1):338. doi: 10.1186/s13054-015-1048-9. Crit Care. 2015. PMID: 26369326 Free PMC article.
-
Estimating Ten-Year Trends in Septic Shock Incidence and Mortality in United States Academic Medical Centers Using Clinical Data.Chest. 2017 Feb;151(2):278-285. doi: 10.1016/j.chest.2016.07.010. Epub 2016 Jul 22. Chest. 2017. PMID: 27452768 Free PMC article.
-
Impact of Policies on the Rise in Sepsis Incidence, 2000-2010.Clin Infect Dis. 2016 Mar 15;62(6):695-703. doi: 10.1093/cid/civ1019. Epub 2016 Jan 19. Clin Infect Dis. 2016. PMID: 26787173 Free PMC article. Review.
-
Sepsis trends: increasing incidence and decreasing mortality, or changing denominator?J Thorac Dis. 2020 Feb;12(Suppl 1):S89-S100. doi: 10.21037/jtd.2019.12.51. J Thorac Dis. 2020. PMID: 32148931 Free PMC article. Review.
Cited by
-
A National Approach to Pediatric Sepsis Surveillance.Pediatrics. 2019 Dec;144(6):e20191790. doi: 10.1542/peds.2019-1790. Pediatrics. 2019. PMID: 31776196 Free PMC article.
-
The Surviving Sepsis Campaign: research priorities for the administration, epidemiology, scoring and identification of sepsis.Intensive Care Med Exp. 2021 Jul 2;9(1):34. doi: 10.1186/s40635-021-00400-z. Intensive Care Med Exp. 2021. PMID: 34212256 Free PMC article. Review.
-
Recognition and Management of Hospital-Acquired Sepsis Among Older General Medical Inpatients: A Multi-Site Retrospective Study.Int J Gen Med. 2023 Mar 21;16:1039-1046. doi: 10.2147/IJGM.S400839. eCollection 2023. Int J Gen Med. 2023. PMID: 36987405 Free PMC article.
-
Application of the Sepsis-3 criteria to describe sepsis epidemiology in the Amsterdam UMCdb intensive care dataset.PLoS One. 2024 Jun 21;19(6):e0304133. doi: 10.1371/journal.pone.0304133. eCollection 2024. PLoS One. 2024. PMID: 38905261 Free PMC article.
-
Diagnosing sepsis is subjective and highly variable: a survey of intensivists using case vignettes.Crit Care. 2016 Apr 6;20:89. doi: 10.1186/s13054-016-1266-9. Crit Care. 2016. PMID: 27048508 Free PMC article.
References
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–54. - PubMed
-
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003. Crit Care Med. 2007;35:1244–50. - PubMed
-
- Kumar G, Kumar N, Taneja A, et al. Nationwide trends of severe sepsis in the 21st century (2000–2007) Chest. 2011;140:1223–31. - PubMed
-
- Hall MJ, Williams SN, DeFrances CJ, Golosinskiy A. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011;62:1–8. - PubMed
-
- Danai PA, Moss M, Mannino DM, Martin GS. The epidemiology of sepsis in patients with malignancy. Chest. 2006;129:1432–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
