

Combination cediranib and olaparib versus olaparib alone for women with recurrent platinum-sensitive ovarian cancer: a randomised phase 2 study
- PMID: 25218906
- PMCID: PMC4294183
- DOI: 10.1016/S1470-2045(14)70391-2
Combination cediranib and olaparib versus olaparib alone for women with recurrent platinum-sensitive ovarian cancer: a randomised phase 2 study
Abstract
Background: Olaparib is a poly(ADP-ribose) polymerase inhibitor and cediranib is an anti-angiogenic agent with activity against VEGF receptor (VEGFR) 1, VEGFR2, and VEGFR3. Both oral agents have antitumour activity in women with recurrent ovarian cancer, and their combination was active and had manageable toxicities in a phase 1 trial. We investigated whether this combination could improve progression-free survival (PFS) compared with olaparib monotherapy in women with recurrent platinum-sensitive ovarian cancer.
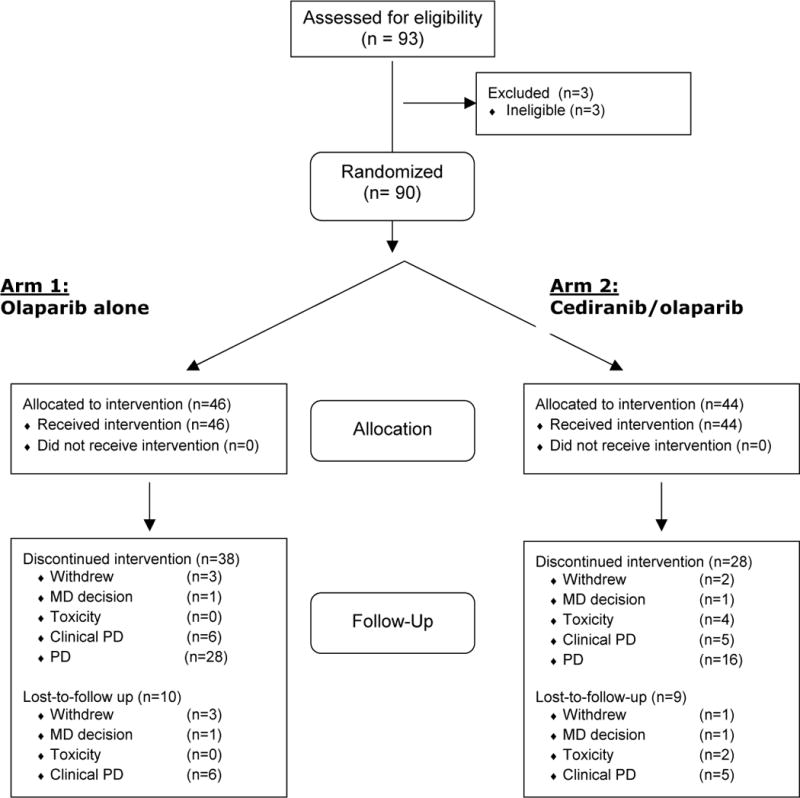
Methods: In our randomised, open-label, phase 2 study, we recruited women (aged ≥18 years) who had measurable platinum-sensitive, relapsed, high-grade serous or endometrioid ovarian, fallopian tube, or primary peritoneal cancer, or those with deleterious germline BRCA1/2 mutations from nine participating US academic medical centres. We randomly allocated participants (1:1) according to permuted blocks, stratified by germline BRCA status and previous anti-angiogenic therapy, to receive olaparib capsules 400 mg twice daily or the combination at the recommended phase 2 dose of cediranib 30 mg daily and olaparib capsules 200 mg twice daily. The primary endpoint was progression-free survival analysed in the intention-to-treat population. The phase 2 trial is no longer accruing patients. An interim analysis was conducted in November, 2013, after 50% of expected events had occurred and efficacy results were unmasked. The primary analysis was performed on March 31, 2014, after 47 events (66% of those expected). The trial is registered with ClinicalTrials.gov, number NCT01116648.
Findings: Between Oct 26, 2011, and June 3, 2013, we randomly allocated 46 women to receive olaparib alone and 44 to receive the combination of olaparib and cediranib. Median PFS was 17·7 months (95% CI 14·7-not reached) for the women treated with cediranib plus olaparib compared with 9·0 months (95% CI 5·7-16·5) for those treated with olaparib monotherapy (hazard ratio 0·42, 95% CI 0·23-0·76; p=0·005). Grade 3 and 4 adverse events were more common with combination therapy than with monotherapy, including fatigue (12 patients in the cediranib plus olaparib group vs five patients in the olaparib monotherapy group), diarrhoea (ten vs none), and hypertension (18 vs none).
Interpretation: Cediranib plus olaparib seems to improve PFS in women with recurrent platinum-sensitive high-grade serous or endometrioid ovarian cancer, and warrants study in a phase 3 trial. The side-effect profile suggests such investigations should include assessments of quality of life and patient-reported outcomes to understand the effects of a continuing oral regimen with that of intermittent chemotherapy.
Funding: American Recovery and Reinvestment Act grant from the National Institutes of Health (NIH) (3 U01 CA062490-16S2); Intramural Program of the Center for Cancer Research; and the Division of Cancer Treatment and Diagnosis, National Cancer Institute, NIH.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare they have no conflicts of interest.
Comment in
-
Combining targeted therapies in ovarian cancer.Lancet Oncol. 2014 Oct;15(11):1179-81. doi: 10.1016/S1470-2045(14)70421-8. Epub 2014 Sep 10. Lancet Oncol. 2014. PMID: 25218905 No abstract available.
Similar articles
-
Overall survival and updated progression-free survival outcomes in a randomized phase II study of combination cediranib and olaparib versus olaparib in relapsed platinum-sensitive ovarian cancer.Ann Oncol. 2019 Apr 1;30(4):551-557. doi: 10.1093/annonc/mdz018. Ann Oncol. 2019. PMID: 30753272 Free PMC article. Clinical Trial.
-
Olaparib combined with chemotherapy for recurrent platinum-sensitive ovarian cancer: a randomised phase 2 trial.Lancet Oncol. 2015 Jan;16(1):87-97. doi: 10.1016/S1470-2045(14)71135-0. Epub 2014 Dec 4. Lancet Oncol. 2015. PMID: 25481791 Clinical Trial.
-
A Phase 1 trial of the poly(ADP-ribose) polymerase inhibitor olaparib (AZD2281) in combination with the anti-angiogenic cediranib (AZD2171) in recurrent epithelial ovarian or triple-negative breast cancer.Eur J Cancer. 2013 Sep;49(14):2972-8. doi: 10.1016/j.ejca.2013.05.020. Epub 2013 Jun 27. Eur J Cancer. 2013. PMID: 23810467 Free PMC article. Clinical Trial.
-
Cediranib, a pan-VEGFR inhibitor, and olaparib, a PARP inhibitor, in combination therapy for high grade serous ovarian cancer.Expert Opin Investig Drugs. 2016;25(5):597-611. doi: 10.1517/13543784.2016.1156857. Epub 2016 Mar 16. Expert Opin Investig Drugs. 2016. PMID: 26899229 Review.
-
Poly(ADP-ribose) polymerase (PARP) inhibitors for the treatment of ovarian cancer.Cochrane Database Syst Rev. 2022 Feb 16;2(2):CD007929. doi: 10.1002/14651858.CD007929.pub4. Cochrane Database Syst Rev. 2022. PMID: 35170751 Free PMC article. Review.
Cited by
-
A Phase I study of olaparib and irinotecan in patients with colorectal cancer: Canadian Cancer Trials Group IND 187.Invest New Drugs. 2016 Aug;34(4):450-7. doi: 10.1007/s10637-016-0351-x. Epub 2016 Apr 13. Invest New Drugs. 2016. PMID: 27075016 Clinical Trial.
-
Circulating Tumor DNA Dynamics Fail to Predict Efficacy of Poly(ADP-ribose) Polymerase/VEGFR Inhibition in Patients With Heavily Pretreated Advanced Solid Tumors.JCO Precis Oncol. 2024 Feb;8:e2300289. doi: 10.1200/PO.23.00289. JCO Precis Oncol. 2024. PMID: 38412387
-
State-of-the-art strategies for targeting the DNA damage response in cancer.Nat Rev Clin Oncol. 2019 Feb;16(2):81-104. doi: 10.1038/s41571-018-0114-z. Nat Rev Clin Oncol. 2019. PMID: 30356138 Free PMC article. Review.
-
Kinase Inhibitors in the Treatment of Ovarian Cancer: Current State and Future Promises.Cancers (Basel). 2022 Dec 19;14(24):6257. doi: 10.3390/cancers14246257. Cancers (Basel). 2022. PMID: 36551745 Free PMC article. Review.
-
Current status and future prospects of PARP inhibitor clinical trials in ovarian cancer.Cancer Manag Res. 2019 May 10;11:4371-4390. doi: 10.2147/CMAR.S200524. eCollection 2019. Cancer Manag Res. 2019. PMID: 31191001 Free PMC article.
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA: a cancer journal for clinicians. 2014 Jan-Feb;64(1):9–29. - PubMed
-
- Jayson GC, Kohn EC, Kitchener HC, Ledermann JA. Ovarian cancer. Lancet. 2014 Apr 17; [Epub ahead of print] - PubMed
-
- Bryant HE, Schultz N, Thomas HD, et al. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature. 2005 Apr 14;434(7035):913–7. - PubMed
-
- Farmer H, McCabe N, Lord CJ, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature. 2005 Apr 14;434(7035):917–21. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
