

The pathogenesis of focal segmental glomerulosclerosis
- PMID: 25168829
- PMCID: PMC4149756
- DOI: 10.1053/j.ackd.2014.05.009
The pathogenesis of focal segmental glomerulosclerosis
Abstract
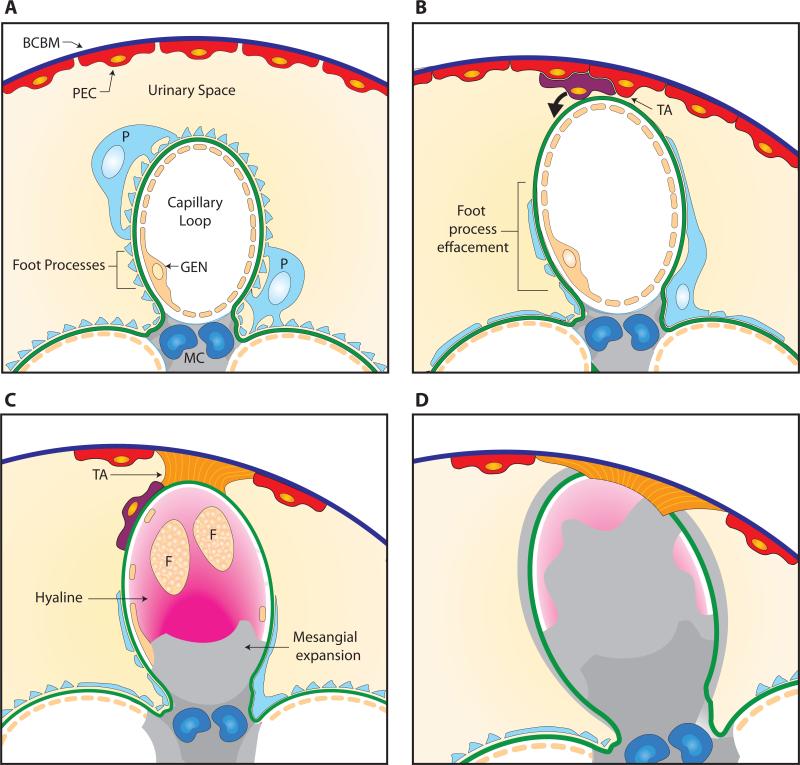
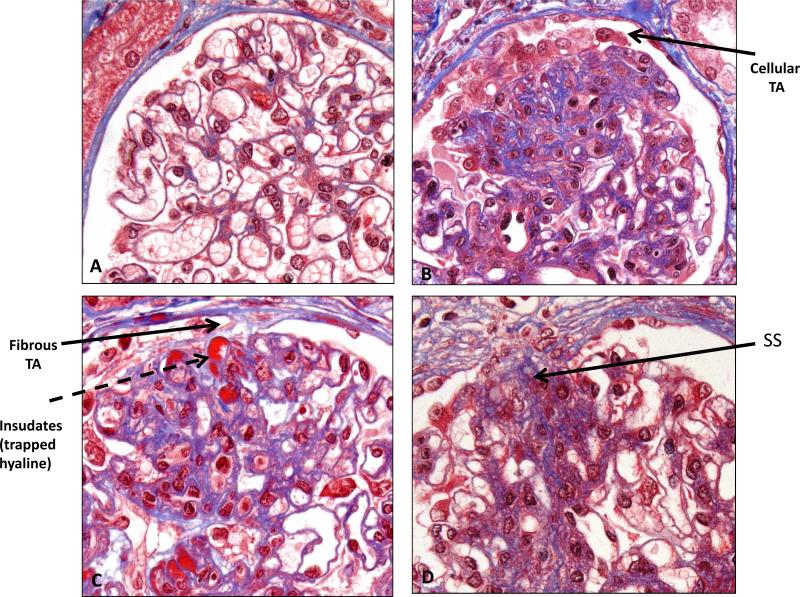
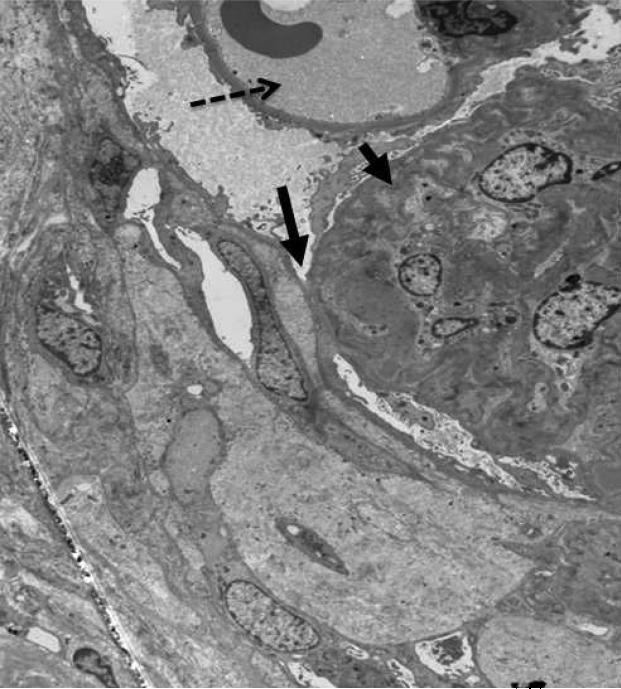
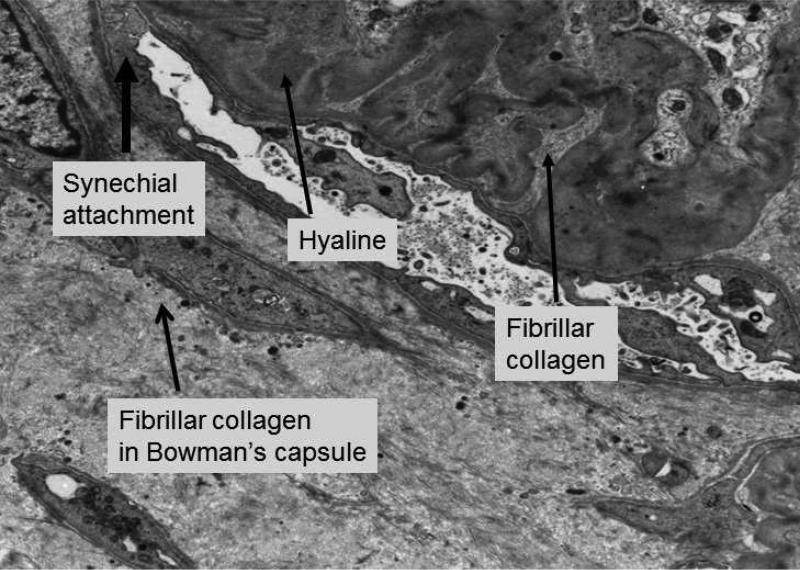
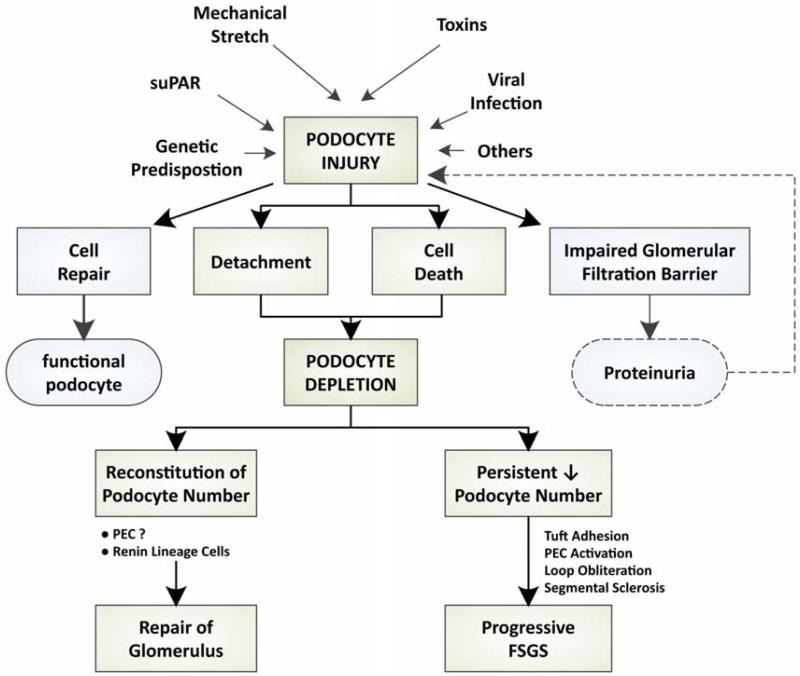
Focal segmental glomerulosclerosis (FSGS) is a histologic pattern of injury on kidney biopsy that can arise from a diverse range of causes and mechanisms. Although primary and secondary forms are described based on the underlying cause, there are many common factors that underlie the development of this segmental injury. In this review, we will describe the currently accepted model for the pathogenesis of classic FSGS and review the data supporting this model. Although the podocyte is considered the major target of injury in FSGS, we will also highlight the contributions of other resident glomerular cells in the development of FSGS.
Keywords: Focal segmental glomerulosclerosis; Glomerular disease; Parietal epithelial cell; Podocyte; Proteinuria.
Copyright © 2014 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Focal and segmental glomerulosclerosis in murine models: a histological and ultrastructural characterization with immunohistochemistry correlation of glomerular CD44 and WT1 expression.Ultrastruct Pathol. 2018 Sep-Oct;42(5):430-439. doi: 10.1080/01913123.2018.1501125. Epub 2018 Oct 4. Ultrastruct Pathol. 2018. PMID: 30285525
-
Mechanisms of Scarring in Focal Segmental Glomerulosclerosis.J Histochem Cytochem. 2019 Sep;67(9):623-632. doi: 10.1369/0022155419850170. Epub 2019 May 22. J Histochem Cytochem. 2019. PMID: 31116068 Free PMC article. Review.
-
The role of podocyte injury in the pathogenesis of focal segmental glomerulosclerosis.Ren Fail. 2000 Nov;22(6):663-84. doi: 10.1081/jdi-100101955. Ren Fail. 2000. PMID: 11104157 Review.
-
Identification of glomerular and podocyte-specific genes and pathways activated by sera of patients with focal segmental glomerulosclerosis.PLoS One. 2019 Oct 3;14(10):e0222948. doi: 10.1371/journal.pone.0222948. eCollection 2019. PLoS One. 2019. PMID: 31581251 Free PMC article.
-
Focal segmental glomerulosclerosis; why does it occur segmentally?Pflugers Arch. 2017 Aug;469(7-8):983-988. doi: 10.1007/s00424-017-2023-x. Epub 2017 Jun 29. Pflugers Arch. 2017. PMID: 28664408 Review.
Cited by
-
INF2 formin variants linked to human inherited kidney disease reprogram the transcriptome, causing mitotic chaos and cell death.Cell Mol Life Sci. 2024 Jun 25;81(1):279. doi: 10.1007/s00018-024-05323-y. Cell Mol Life Sci. 2024. PMID: 38916773 Free PMC article.
-
Physiologically-based pharmacokinetic model of sparsentan to evaluate drug-drug interaction potential.CPT Pharmacometrics Syst Pharmacol. 2024 Feb;13(2):317-329. doi: 10.1002/psp4.13086. Epub 2023 Dec 2. CPT Pharmacometrics Syst Pharmacol. 2024. PMID: 38041499 Free PMC article.
-
Physiological Replication of the Human Glomerulus Using a Triple Culture Microphysiological System.Adv Sci (Weinh). 2023 Nov;10(33):e2303131. doi: 10.1002/advs.202303131. Epub 2023 Oct 22. Adv Sci (Weinh). 2023. PMID: 37867234 Free PMC article.
-
Focal Segmental Glomerulosclerosis and Hyalinosis in a Patient with Spondyloarthritis: A Rare Renal Involvement Case Report.Mediterr J Rheumatol. 2023 Jun 30;34(2):257-261. doi: 10.31138/mjr.34.2.257. eCollection 2023 Jun. Mediterr J Rheumatol. 2023. PMID: 37654640 Free PMC article.
-
Extracellular vesicles from focal segmental glomerulosclerosis pediatric patients induce STAT3 activation and mesangial cell proliferation.PLoS One. 2022 Nov 14;17(11):e0274598. doi: 10.1371/journal.pone.0274598. eCollection 2022. PLoS One. 2022. PMID: 36374911 Free PMC article.
References
-
- D'Agati VD, Fogo AB, Bruijn JA, et al. Pathologic classification of focal segmental glomerulosclerosis: a working proposal. Am J Kidney Dis. 2004;43:368–382. - PubMed
-
- Kriz W, Elger M, Nagata M, et al. The role of podocytes in the development of glomerular TE sclerosis. Kidney Int Suppl. 1994;45:S64–72. - PubMed
-
- LeHir M, Kriz W. New insights into structural patterns encountered in glomerulosclerosis. Curr Opin Nephrol Hypertens. 2007;16:184–191. - PubMed
-
- Verani RR, Hawkins EP. Recurrent focal segmental glomerulosclerosis. A pathological study of the early lesion. Am J Nephrol. 1986;6:263–270. - PubMed
-
- Rood IM, Deegens JK, Wetzels JF. Genetic causes of focal segmental glomerulosclerosis: implications for clinical practice. Nephrol Dial Transplant. 2012;27:882–890. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
