

The role of microglia in human disease: therapeutic tool or target?
- PMID: 25107477
- PMCID: PMC4131134
- DOI: 10.1007/s00401-014-1330-y
The role of microglia in human disease: therapeutic tool or target?
Abstract
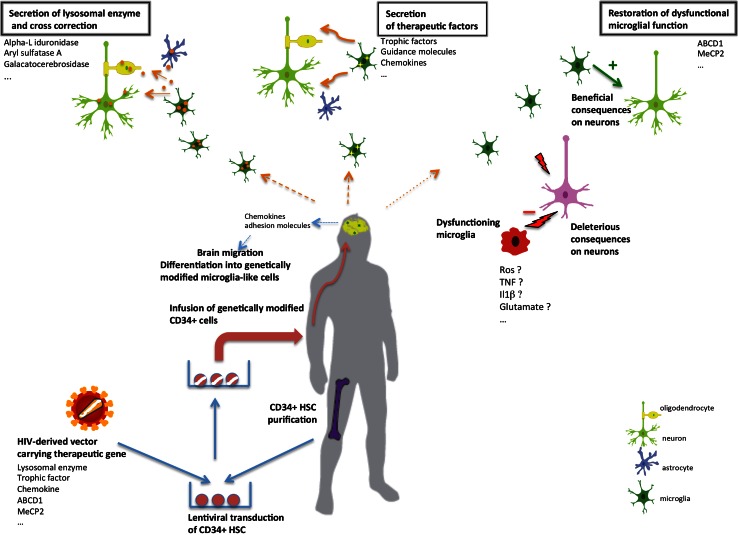
Microglia have long been the focus of much attention due to their strong proliferative response (microgliosis) to essentially any kind of damage to the CNS. More recently, we reached the realization that these cells play specific roles in determining progression and outcomes of essentially all CNS disease. Thus, microglia has ceased to be viewed as an accessory to underlying pathologies and has now taken center stage as a therapeutic target. Here, we review how our understanding of microglia's involvement in promoting or limiting the pathogenesis of diseases such as amyotrophic lateral sclerosis, Alzheimer's disease, Huntington's disease, multiple sclerosis, X-linked adrenoleukodystrophy (X-ALD) and lysosomal storage diseases (LSD) has changed over time. While strategies to suppress the deleterious and promote the virtuous functions of microglia will undoubtedly be forthcoming, replacement of these cells has already proven its usefulness in a clinical setting. Over the past few years, we have reached the realization that microglia have a developmental origin that is distinct from that of bone marrow-derived myelomonocytic cells. Nevertheless, microglia can be replaced, in specific situations, by the progeny of hematopoietic stem cells (HSCs), pointing to a strategy to engineer the CNS environment through the transplantation of modified HSCs. Thus, microglia replacement has been successfully exploited to deliver therapeutics to the CNS in human diseases such as X-ALD and LSD. With this outlook in mind, we will discuss the evidence existing so far for microglial involvement in the pathogenesis and the therapy of specific CNS disease.
Figures
Similar articles
-
Microglia as therapeutic target in central nervous system disorders.J Pharmacol Sci. 2020 Nov;144(3):102-118. doi: 10.1016/j.jphs.2020.07.004. Epub 2020 Aug 15. J Pharmacol Sci. 2020. PMID: 32921391 Review.
-
Monitoring disease evolution and treatment response in lysosomal disorders by the peripheral benzodiazepine receptor ligand PK11195.Neurobiol Dis. 2009 Apr;34(1):51-62. doi: 10.1016/j.nbd.2008.12.019. Neurobiol Dis. 2009. PMID: 19320046
-
Microglia in Health and Disease.Cold Spring Harb Perspect Biol. 2015 Sep 9;8(1):a020560. doi: 10.1101/cshperspect.a020560. Cold Spring Harb Perspect Biol. 2015. PMID: 26354893 Free PMC article. Review.
-
Microglia in health and disease.J Neurosci Res. 2005 Aug 1;81(3):302-13. doi: 10.1002/jnr.20562. J Neurosci Res. 2005. PMID: 15954124 Review.
-
Unique molecular signature in mucolipidosis type IV microglia.J Neuroinflammation. 2019 Dec 28;16(1):276. doi: 10.1186/s12974-019-1672-4. J Neuroinflammation. 2019. PMID: 31883529 Free PMC article.
Cited by
-
iPSC-Derived Macrophages Effectively Treat Pulmonary Alveolar Proteinosis in Csf2rb-Deficient Mice.Stem Cell Reports. 2018 Sep 11;11(3):696-710. doi: 10.1016/j.stemcr.2018.07.006. Epub 2018 Aug 9. Stem Cell Reports. 2018. PMID: 30100408 Free PMC article.
-
Gestational Hypothyroxinemia Imprints a Switch in the Capacity of Astrocytes and Microglial Cells of the Offspring to React in Inflammation.Mol Neurobiol. 2018 May;55(5):4373-4387. doi: 10.1007/s12035-017-0627-y. Epub 2017 Jun 27. Mol Neurobiol. 2018. PMID: 28656482
-
Regulatory effects of caffeic acid phenethyl ester on neuroinflammation in microglial cells.Int J Mol Sci. 2015 Mar 11;16(3):5572-89. doi: 10.3390/ijms16035572. Int J Mol Sci. 2015. PMID: 25768341 Free PMC article.
-
Brain Metabolic Alterations in Alzheimer's Disease.Int J Mol Sci. 2022 Mar 29;23(7):3785. doi: 10.3390/ijms23073785. Int J Mol Sci. 2022. PMID: 35409145 Free PMC article. Review.
-
Competitive repopulation of an empty microglial niche yields functionally distinct subsets of microglia-like cells.Nat Commun. 2018 Nov 19;9(1):4845. doi: 10.1038/s41467-018-07295-7. Nat Commun. 2018. PMID: 30451869 Free PMC article.
References
-
- Abbott NJ, Patabendige AA, Dolman DE, et al. Structure and function of the blood-brain barrier. Neurobiol Dis. 2010;37:13–25. - PubMed
-
- Ajami B, Bennett JL, Krieger C, et al. Local self-renewal can sustain CNS microglia maintenance and function throughout adult life. Nat Neurosci. 2007;10:1538–1543. - PubMed
-
- Ajami B, Bennett JL, Krieger C, et al. Infiltrating monocytes trigger EAE progression, but do not contribute to the resident microglia pool. Nat Neurosci. 2011;14:1142–1149. - PubMed
-
- Alliot F, Godin I, Pessac B. Microglia derive from progenitors, originating from the yolk sac, and which proliferate in the brain. Brain Res Dev Brain Res. 1999;117:145–152. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
