

Disparities in perceived unmet need for supportive services among patients with lung cancer in the Cancer Care Outcomes Research and Surveillance Consortium
- PMID: 24985538
- PMCID: PMC4414401
- DOI: 10.1002/cncr.28801
Disparities in perceived unmet need for supportive services among patients with lung cancer in the Cancer Care Outcomes Research and Surveillance Consortium
Abstract
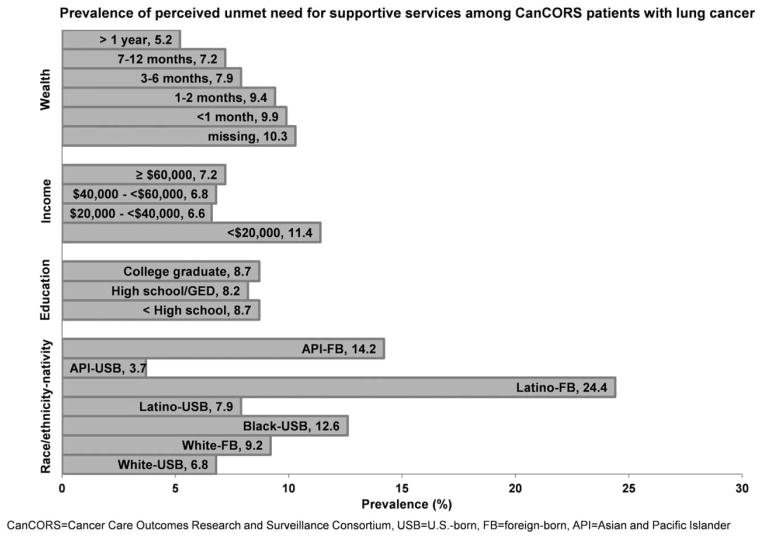
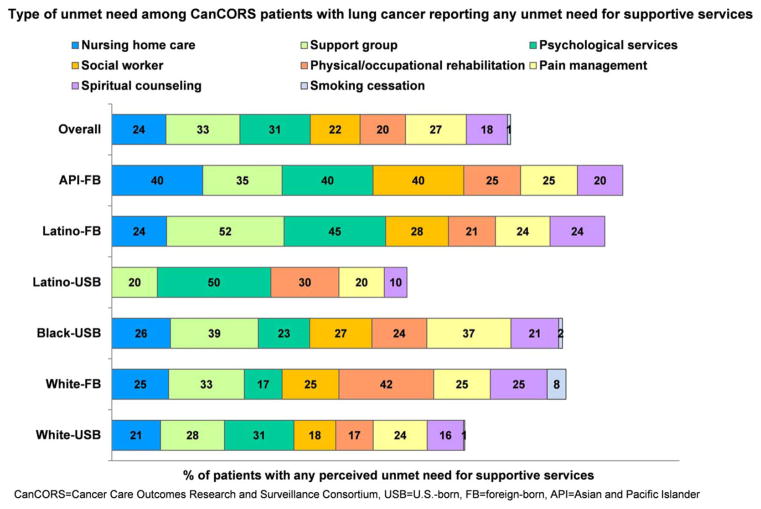
Background: The authors investigated the prevalence, determinants of, and disparities in any perceived unmet need for 8 supportive services (home nurse, support group, psychological services, social worker, physical/occupational rehabilitation, pain management, spiritual counseling, and smoking cessation) by race/ethnicity and nativity and how it is associated with perceived quality of care among US patients with lung cancer.
Methods: Data from a multiregional, multihealth system representative cohort of 4334 newly diagnosed patients were analyzed. Binomial logistic regression models adjusted for patient clustering.
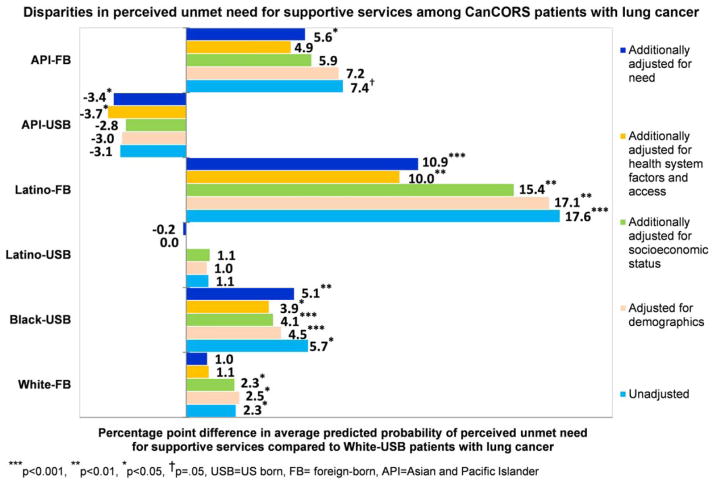
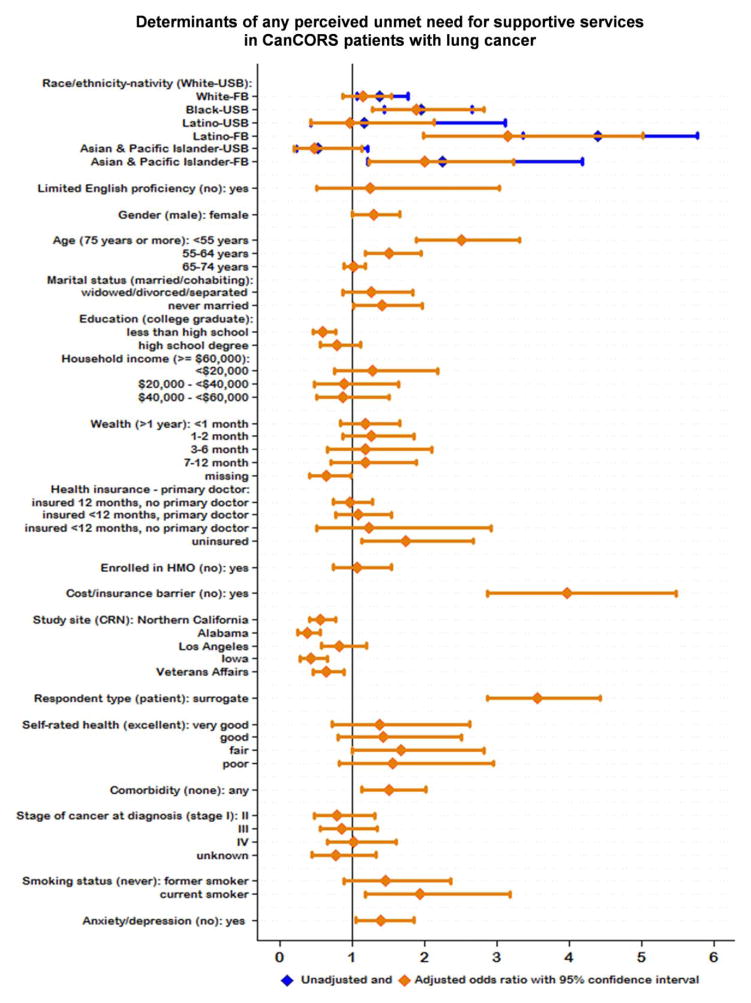
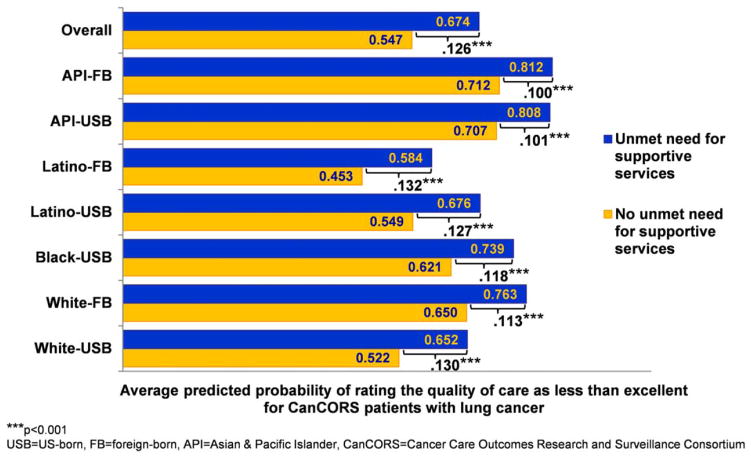
Results: Patients with any perceived unmet need (9% overall) included 7% of white-US-born (USB), 9% of white-foreign-born (FB), 13% of black-USB, 8% of Latino-USB, 24% of Latino-FB, 4% of Asian/Pacific Islander (API)-USB, 14% of API-FB, and 11% of "other" patients (P < .001). Even after controlling for demographic and socioeconomic factors, health system and health care access, and need, black-USB, Latino-FB, and Asian-FB patients were more likely to perceive an unmet need than white-USB patients by 5.1, 10.9, and 5.6 percentage points, respectively (all P < .05). Being younger, female, never married, uninsured, a current smoker, or under surrogate care or having comorbidity, anxiety/depression, or a cost/insurance barrier to getting tests/treatments were associated with any unmet need. Patients with any unmet need were more likely to rate care as less-than-"excellent" by 13 percentage points than patients with no unmet need (P < .001).
Conclusions: Significant disparities in unmet supportive service need by race/ethnicity and nativity highlight immigrants with lung cancer as being particularly underserved. Eliminating disparities in access to needed supportive services is essential for delivering patient-centered, equitable cancer care.
Keywords: health care disparities; immigrants; lung cancer; patient-centered care; supportive care; underserved populations.
© 2014 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
The authors made no disclosures apart from the funding sources.
Figures
Similar articles
-
Barriers and unmet need for supportive services for HIV patients in care in Los Angeles County, California.AIDS Patient Care STDS. 2011 Sep;25(9):525-32. doi: 10.1089/apc.2011.0149. Epub 2011 Jul 20. AIDS Patient Care STDS. 2011. PMID: 21774689
-
Disparities in dental insurance coverage and dental care among US children: the National Survey of Children's Health.Pediatrics. 2007 Feb;119 Suppl 1:S12-21. doi: 10.1542/peds.2006-2089D. Pediatrics. 2007. PMID: 17272579
-
Quality of cancer care among foreign-born and US-born patients with lung or colorectal cancer.Cancer. 2010 Dec 1;116(23):5497-506. doi: 10.1002/cncr.25546. Epub 2010 Jul 29. Cancer. 2010. PMID: 20672356 Free PMC article.
-
An official American Thoracic Society systematic review: insurance status and disparities in lung cancer practices and outcomes.Am J Respir Crit Care Med. 2010 Nov 1;182(9):1195-205. doi: 10.1164/rccm.2009-038ST. Am J Respir Crit Care Med. 2010. PMID: 21041563 Review.
-
What are the unmet supportive care needs of people with cancer? A systematic review.Support Care Cancer. 2009 Aug;17(8):1117-28. doi: 10.1007/s00520-009-0615-5. Epub 2009 Mar 25. Support Care Cancer. 2009. PMID: 19319577 Review.
Cited by
-
Investigation of Racial Disparities in Early Supportive Medication Use and End-of-Life Care Among Medicare Beneficiaries With Stage IV Breast Cancer.J Clin Oncol. 2016 Jul 1;34(19):2265-70. doi: 10.1200/JCO.2015.64.8162. Epub 2016 May 9. J Clin Oncol. 2016. PMID: 27161968 Free PMC article.
-
Lower Patient Ratings of Physician Communication Are Associated With Unmet Need for Symptom Management in Patients With Lung and Colorectal Cancer.J Oncol Pract. 2016 Jun;12(6):e654-69. doi: 10.1200/JOP.2015.005538. Epub 2016 May 24. J Oncol Pract. 2016. PMID: 27221991 Free PMC article.
-
Investigating racial disparities in use of NK1 receptor antagonists to prevent chemotherapy-induced nausea and vomiting among women with breast cancer.Breast Cancer Res Treat. 2016 Apr;156(2):351-9. doi: 10.1007/s10549-016-3747-6. Epub 2016 Mar 11. Breast Cancer Res Treat. 2016. PMID: 26968396 Free PMC article.
-
Effects of oriental medicine music therapy in an ovarian cancer patient with So-Eum-type constitution: a case report.Integr Med Res. 2015 Mar;4(1):48-52. doi: 10.1016/j.imr.2014.12.002. Epub 2014 Dec 31. Integr Med Res. 2015. PMID: 28664109 Free PMC article.
-
Policies and Practices to Address Cancer's Long-Term Adverse Consequences.J Natl Cancer Inst. 2022 Aug 8;114(8):1065-1071. doi: 10.1093/jnci/djac086. J Natl Cancer Inst. 2022. PMID: 35438165 Free PMC article.
References
-
- American Cancer Society. Cancer Facts & Figures 2012. Atlanta, GA: American Cancer Society; 2012.
-
- Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. The prevalence of psychological distress by cancer site. Psychooncology. 2001;10:19–28. - PubMed
-
- Carlsen K, Jensen AB, Jacobsen E, Krasnik M, Johansen C. Psychosocial aspects of lung cancer. Lung Cancer. 2005;47:293–300. - PubMed
Publication types
MeSH terms
Grants and funding
- U01CA093339/CA/NCI NIH HHS/United States
- U01CA093329/CA/NCI NIH HHS/United States
- U01 CA093348/CA/NCI NIH HHS/United States
- U01CA093344/CA/NCI NIH HHS/United States
- U01 CA093339/CA/NCI NIH HHS/United States
- U01 CA093344/CA/NCI NIH HHS/United States
- U01 CA093326/CA/NCI NIH HHS/United States
- P50 CA148596/CA/NCI NIH HHS/United States
- U01CA093326/CA/NCI NIH HHS/United States
- P50CA148596/CA/NCI NIH HHS/United States
- U01 CA093329/CA/NCI NIH HHS/United States
- U01 CA093324/CA/NCI NIH HHS/United States
- U01CA093324/CA/NCI NIH HHS/United States
- U01 CA093332/CA/NCI NIH HHS/United States
- U01CA093348/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
