

Brain distribution of dipeptide repeat proteins in frontotemporal lobar degeneration and motor neurone disease associated with expansions in C9ORF72
- PMID: 24950788
- PMCID: PMC4229740
- DOI: 10.1186/2051-5960-2-70
Brain distribution of dipeptide repeat proteins in frontotemporal lobar degeneration and motor neurone disease associated with expansions in C9ORF72
Abstract
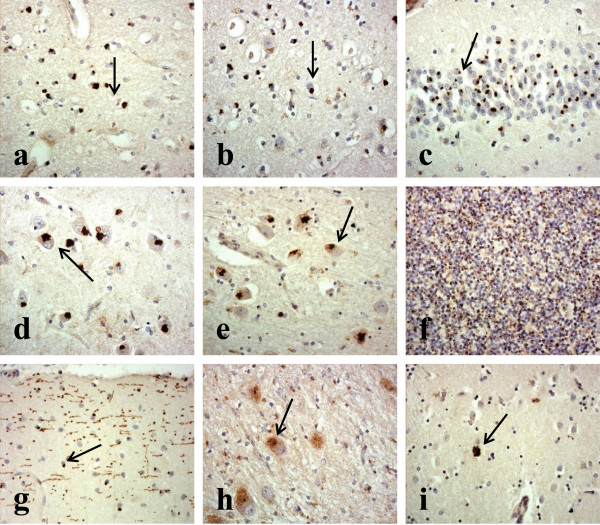
A hexanucleotide (GGGGCC) expansion in C9ORF72 gene is the most common genetic change seen in familial Frontotemporal Lobar Degeneration (FTLD) and familial Motor Neurone Disease (MND). Pathologically, expansion bearers show characteristic p62 positive, TDP-43 negative inclusion bodies within cerebellar and hippocampal neurons which also contain dipeptide repeat proteins (DPR) formed from sense and antisense RAN (repeat associated non ATG-initiated) translation of the expanded repeat region itself. 'Inappropriate' formation, and aggregation, of DPR might therefore confer neurotoxicity and influence clinical phenotype. Consequently, we compared the topographic brain distribution of DPR in 8 patients with Frontotemporal dementia (FTD), 6 with FTD + MND and 7 with MND alone (all 21 patients bearing expansions in C9ORF72) using a polyclonal antibody to poly-GA, and related this to the extent of TDP-43 pathology in key regions of cerebral cortex and hippocampus. There were no significant differences in either the pattern or severity of brain distribution of DPR between FTD, FTD + MND and MND groups, nor was there any relationship between the distribution of DPR and TDP-43 pathologies in expansion bearers. Likewise, there were no significant differences in the extent of TDP-43 pathology between FTLD patients bearing an expansion in C9ORF72 and non-bearers of the expansion. There were no association between the extent of DPR pathology and TMEM106B or APOE genotypes. However, there was a negative correlation between the extent of DPR pathology and age at onset. Present findings therefore suggest that although the presence and topographic distribution of DPR may be of diagnostic relevance in patients bearing expansion in C9ORF72 this has no bearing on the determination of clinical phenotype. Because TDP-43 pathologies are similar in bearers and non-bearers of the expansion, the expansion may act as a major genetic risk factor for FTLD and MND by rendering the brain highly vulnerable to those very same factors which generate FTLD and MND in sporadic disease.
Figures

Similar articles
-
Accumulation of dipeptide repeat proteins predates that of TDP-43 in frontotemporal lobar degeneration associated with hexanucleotide repeat expansions in C9ORF72 gene.Neuropathol Appl Neurobiol. 2015 Aug;41(5):601-12. doi: 10.1111/nan.12178. Epub 2015 Apr 30. Neuropathol Appl Neurobiol. 2015. PMID: 25185840 Free PMC article.
-
Dipeptide repeat proteins are present in the p62 positive inclusions in patients with frontotemporal lobar degeneration and motor neurone disease associated with expansions in C9ORF72.Acta Neuropathol Commun. 2013 Oct 14;1:68. doi: 10.1186/2051-5960-1-68. Acta Neuropathol Commun. 2013. PMID: 24252525 Free PMC article.
-
Neurodegeneration in frontotemporal lobar degeneration and motor neurone disease associated with expansions in C9orf72 is linked to TDP-43 pathology and not associated with aggregated forms of dipeptide repeat proteins.Neuropathol Appl Neurobiol. 2016 Apr;42(3):242-54. doi: 10.1111/nan.12292. Epub 2015 Dec 7. Neuropathol Appl Neurobiol. 2016. PMID: 26538301 Free PMC article.
-
The neuropathology associated with repeat expansions in the C9ORF72 gene.Acta Neuropathol. 2014 Mar;127(3):347-57. doi: 10.1007/s00401-013-1232-4. Epub 2013 Dec 20. Acta Neuropathol. 2014. PMID: 24356984 Review.
-
Current insights into the C9orf72 repeat expansion diseases of the FTLD/ALS spectrum.Trends Neurosci. 2013 Aug;36(8):450-9. doi: 10.1016/j.tins.2013.04.010. Epub 2013 Jun 7. Trends Neurosci. 2013. PMID: 23746459 Review.
Cited by
-
Loss of Tmem106b is unable to ameliorate frontotemporal dementia-like phenotypes in an AAV mouse model of C9ORF72-repeat induced toxicity.Acta Neuropathol Commun. 2018 May 31;6(1):42. doi: 10.1186/s40478-018-0545-x. Acta Neuropathol Commun. 2018. PMID: 29855382 Free PMC article.
-
Repeat-associated non-AUG (RAN) translation: insights from pathology.Lab Invest. 2019 Jul;99(7):929-942. doi: 10.1038/s41374-019-0241-x. Epub 2019 Mar 27. Lab Invest. 2019. PMID: 30918326 Free PMC article. Review.
-
The role of lysosomes and autophagosomes in frontotemporal lobar degeneration.Neuropathol Appl Neurobiol. 2019 Apr;45(3):244-261. doi: 10.1111/nan.12500. Epub 2018 Jun 19. Neuropathol Appl Neurobiol. 2019. PMID: 29790198 Free PMC article.
-
C9orf72 BAC Transgenic Mice Display Typical Pathologic Features of ALS/FTD.Neuron. 2015 Dec 2;88(5):892-901. doi: 10.1016/j.neuron.2015.10.027. Neuron. 2015. PMID: 26637796 Free PMC article.
-
Fluid Biomarkers of Frontotemporal Lobar Degeneration.Adv Exp Med Biol. 2021;1281:123-139. doi: 10.1007/978-3-030-51140-1_9. Adv Exp Med Biol. 2021. PMID: 33433873
References
-
- Hutton M, Lendon CL, Rizzu P, Baker M, Froelich S, Houlden M, Pickering-Brown SM, Chakraverty S, Isaacs A, Grover A, Hackett J, Adamson J, Lincoln S, Dickson D, Davies P, Petersen RC, Stevens M, de Graaf E, Wauters E, van Baren J, Hillebrand M, Joosse M, Kwon JM, Nowotny P, Che LK, Norton J, Morris JC, Reed LA, Trojanowski JQ, Basun H, et al. Coding and splice donor site mutations in tau cause autosomal dominant dementia (FTDP-17) Nature. 1998;393:702–705. doi: 10.1038/31508. - DOI - PubMed
-
- Baker M, Mackenzie IRA, Pickering-Brown SM, Gass J, Rademakers R, Lindholm C, Snowden J, Adamson J, Sadovnick AD, Rollinson S, Cannon A, Dwosh E, Neary D, Melquist S, Richardson A, Dickson D, Eriksen J, Robinson T, Zehr C, Dickey CA, Crook R, McGowan E, Mann D, Boeve B, Feldman H, Hutton M. Mutations in Progranulin cause tau-negative frontotemporal dementia linked to chromosome 17. Nature. 2006;442:916–919. doi: 10.1038/nature05016. - DOI - PubMed
-
- Cruts M, Gijselinck I, van der Zee J, Engelborghs S, Wils H, Pirici D, Rademakers R, Vandenberghe R, Dermaut B, Martin JJ, van Duijn C, Peeters K, Sciot R, Santens P, De Pooter T, Mattheijssens M, Van den Broeck M, Cuijt I, Vennekens K, De Deyn PP, Kumar-Singh S, Van Broeckhoven C. Null mutations in progranulin cause ubiquitin-positive frontotemporal dementia linked to chromosome 17q21. Nature. 2006;442:920–924. doi: 10.1038/nature05017. - DOI - PubMed
-
- Skibinski G, Parkinson NJ, Brown JM, Chakrabarti L, Lloyd SL, Hummerich H, Nielsen JE, Hodges JR, Spillantini MG, Thusgaard T, Brandner S, Brun A, Rossor MN, Gade A, Johannsen P, Sørensen SA, Gydesen S, Fisher EM, Collinge J. Mutations in the endosomal ESCRTIII-complex subunit CHMP2B in frontotemporal dementia. Nat Genet. 2005;37:806–808. doi: 10.1038/ng1609. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
