

Molecular mechanisms of diabetic kidney disease
- PMID: 24892707
- PMCID: PMC4089448
- DOI: 10.1172/JCI72271
Molecular mechanisms of diabetic kidney disease
Abstract
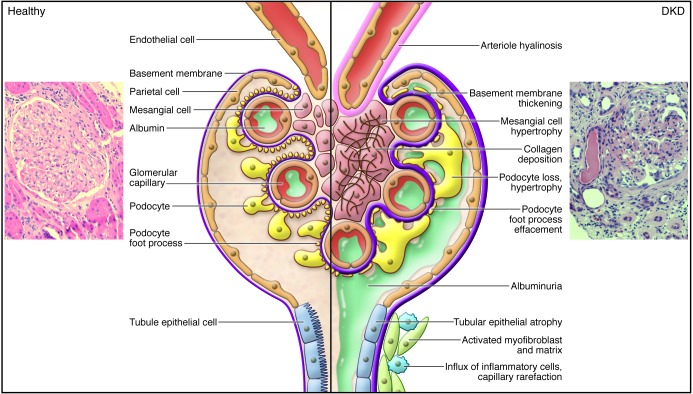
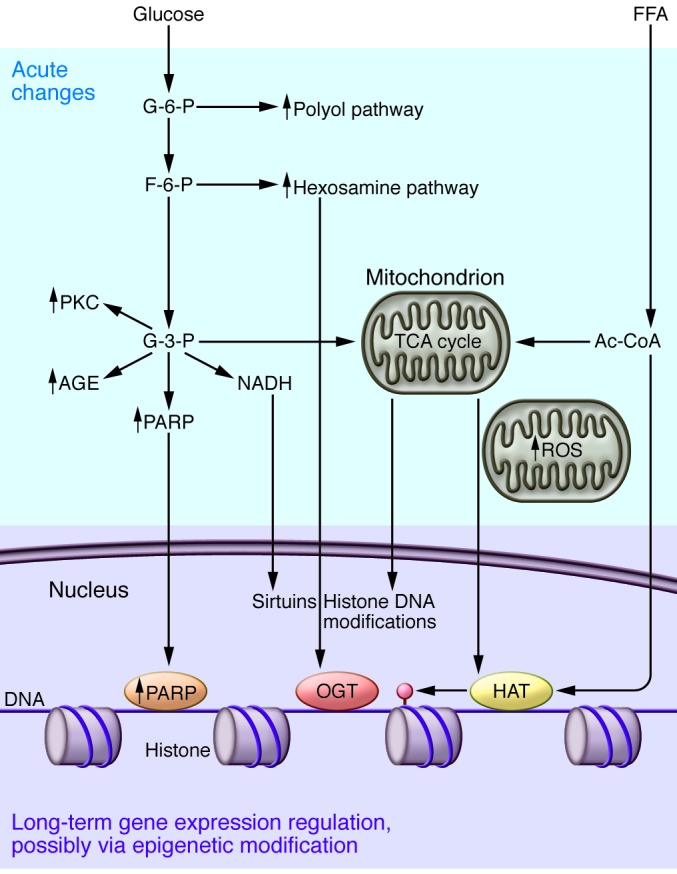
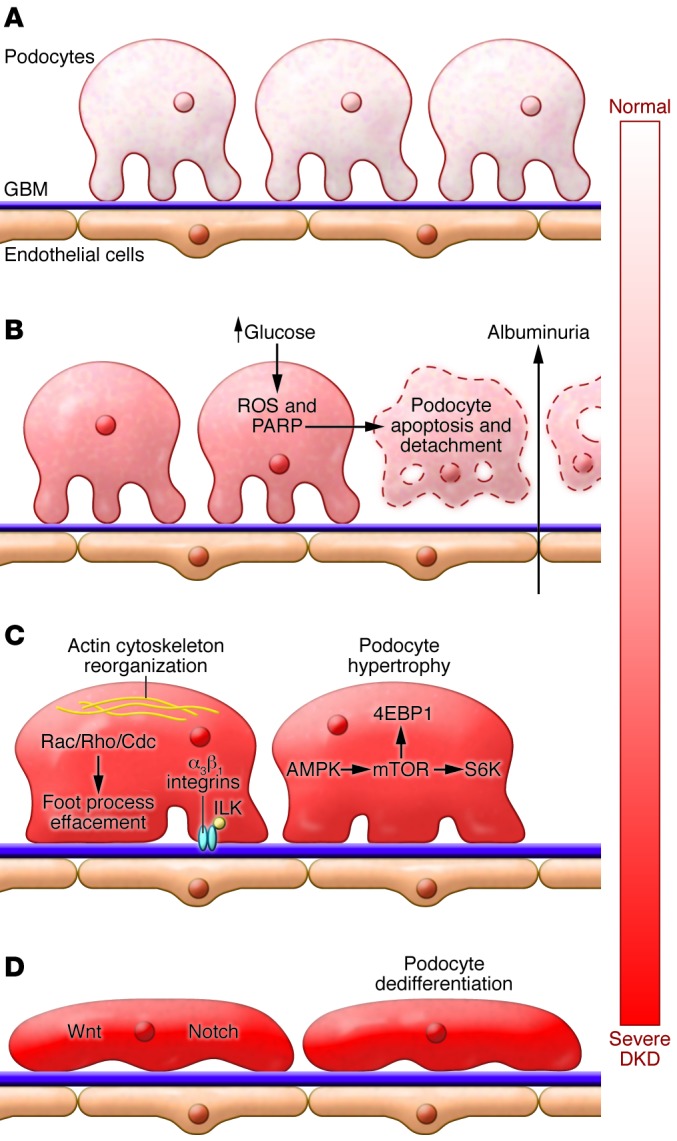
Diabetic kidney disease (DKD) is the leading cause of kidney failure worldwide and the single strongest predictor of mortality in patients with diabetes. DKD is a prototypical disease of gene and environmental interactions. Tight glucose control significantly decreases DKD incidence, indicating that hyperglycemia-induced metabolic alterations, including changes in energy utilization and mitochondrial dysfunction, play critical roles in disease initiation. Blood pressure control, especially with medications that inhibit the angiotensin system, is the only effective way to slow disease progression. While DKD is considered a microvascular complication of diabetes, growing evidence indicates that podocyte loss and epithelial dysfunction play important roles. Inflammation, cell hypertrophy, and dedifferentiation by the activation of classic pathways of regeneration further contribute to disease progression. Concerted clinical and basic research efforts will be needed to understand DKD pathogenesis and to identify novel drug targets.
Figures
Similar articles
-
[Abnormality of renin-angiotensin system in podocyte dysfunction in diabetic kidney disease].Sheng Li Ke Xue Jin Zhan. 2011 Aug;42(4):246-50. Sheng Li Ke Xue Jin Zhan. 2011. PMID: 22066414 Review. Chinese.
-
Molecular Mechanisms in Early Diabetic Kidney Disease: Glomerular Endothelial Cell Dysfunction.Int J Mol Sci. 2020 Dec 11;21(24):9456. doi: 10.3390/ijms21249456. Int J Mol Sci. 2020. PMID: 33322614 Free PMC article. Review.
-
Mechanism of progression of diabetic kidney disease mediated by podocyte mitochondrial injury.Mol Biol Rep. 2020 Oct;47(10):8023-8035. doi: 10.1007/s11033-020-05749-0. Epub 2020 Sep 12. Mol Biol Rep. 2020. PMID: 32918716 Review.
-
Pathogenesis of the podocytopathy and proteinuria in diabetic glomerulopathy.Curr Diabetes Rev. 2008 Feb;4(1):39-45. doi: 10.2174/157339908783502370. Curr Diabetes Rev. 2008. PMID: 18220694 Review.
-
Research advance in the mechanism for oxidative stress-induced podocyte injury in diabetic kidney disease.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021 Dec 28;46(12):1403-1408. doi: 10.11817/j.issn.1672-7347.2021.210199. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021. PMID: 35232911 Free PMC article. Chinese, English.
Cited by
-
Peptide Hormone Insulin Regulates Function, Expression, and SUMOylation of Organic Anion Transporter 3.AAPS J. 2021 Mar 11;23(2):41. doi: 10.1208/s12248-021-00575-z. AAPS J. 2021. PMID: 33709304 Free PMC article.
-
Reversal of the renal hyperglycemic memory in diabetic kidney disease by targeting sustained tubular p21 expression.Nat Commun. 2022 Aug 27;13(1):5062. doi: 10.1038/s41467-022-32477-9. Nat Commun. 2022. PMID: 36030260 Free PMC article.
-
Autophagy in renal fibrosis: Protection or promotion?Front Pharmacol. 2022 Aug 24;13:963920. doi: 10.3389/fphar.2022.963920. eCollection 2022. Front Pharmacol. 2022. PMID: 36105212 Free PMC article. Review.
-
Endothelial SIRT3 regulates myofibroblast metabolic shifts in diabetic kidneys.iScience. 2021 Apr 6;24(5):102390. doi: 10.1016/j.isci.2021.102390. eCollection 2021 May 21. iScience. 2021. PMID: 33981977 Free PMC article.
-
The Contribution of Lipotoxicity to Diabetic Kidney Disease.Cells. 2022 Oct 14;11(20):3236. doi: 10.3390/cells11203236. Cells. 2022. PMID: 36291104 Free PMC article. Review.
References
-
- [No authors listed] USRDS: the United States Renal Data System. Am J Kidney Dis. 2003;42(6 suppl 5):1–230. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
