

Gut epithelial barrier dysfunction and innate immune activation predict mortality in treated HIV infection
- PMID: 24755434
- PMCID: PMC4192038
- DOI: 10.1093/infdis/jiu238
Gut epithelial barrier dysfunction and innate immune activation predict mortality in treated HIV infection
Abstract
Background: While inflammation predicts mortality in treated human immunodeficiency virus (HIV) infection, the prognostic significance of gut barrier dysfunction and phenotypic T-cell markers remains unclear.
Methods: We assessed immunologic predictors of mortality in a case-control study within the Longitudinal Study of the Ocular Complications of AIDS (LSOCA), using conditional logistic regression. Sixty-four case patients who died within 12 months of treatment-mediated viral suppression were each matched to 2 control individuals (total number of controls, 128) by duration of antiretroviral therapy-mediated viral suppression, nadir CD4(+) T-cell count, age, sex, and prior cytomegalovirus (CMV) retinitis. A similar secondary analysis was conducted in the SCOPE cohort, which had participants with less advanced immunodeficiency.
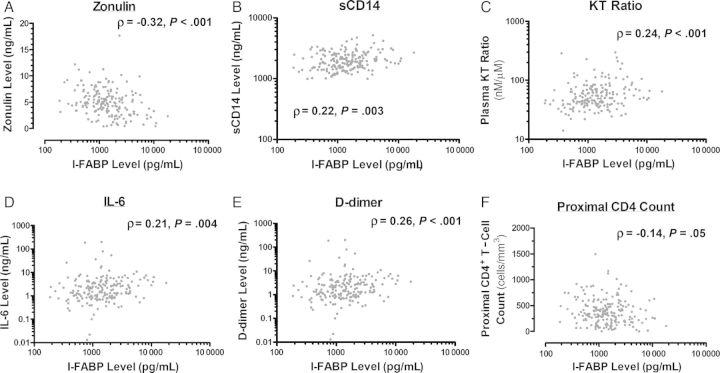
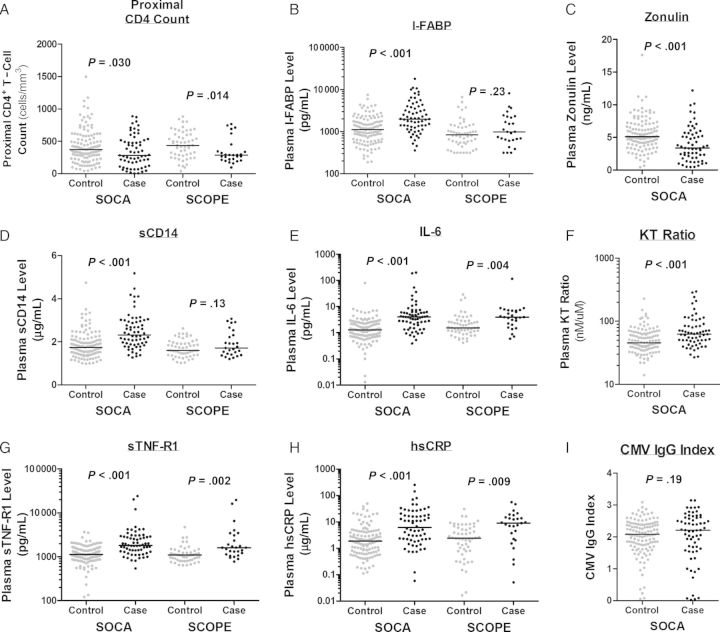
Results: Plasma gut epithelial barrier integrity markers (intestinal fatty acid binding protein and zonulin-1 levels), soluble CD14 level, kynurenine/tryptophan ratio, soluble tumor necrosis factor receptor 1 level, high-sensitivity C-reactive protein level, and D-dimer level all strongly predicted mortality, even after adjustment for proximal CD4(+) T-cell count (all P ≤ .001). A higher percentage of CD38(+)HLA-DR(+) cells in the CD8(+) T-cell population was a predictor of mortality before (P = .031) but not after (P = .10) adjustment for proximal CD4(+) T-cell count. Frequencies of senescent (defined as CD28(-)CD57(+) cells), exhausted (defined as PD1(+) cells), naive, and CMV-specific T cells did not predict mortality.
Conclusions: Gut epithelial barrier dysfunction, innate immune activation, inflammation, and coagulation-but not T-cell activation, senescence, and exhaustion-independently predict mortality in individuals with treated HIV infection with a history of AIDS and are viable targets for interventions.
Keywords: CD28; CD38; CD57; D-dimer; HIV; HLA-DR; IL-6; T-cell activation; antiretroviral therapy; cytomegalovirus; gut epithelial cell barrier; hsCRP; immune activation; intestinal fatty acid binding protein (I-FABP); mortality; sCD14; zonulin-1.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Soluble markers of inflammation and coagulation but not T-cell activation predict non-AIDS-defining morbid events during suppressive antiretroviral treatment.J Infect Dis. 2014 Oct 15;210(8):1248-59. doi: 10.1093/infdis/jiu254. Epub 2014 May 1. J Infect Dis. 2014. PMID: 24795473 Free PMC article.
-
HIV-infected individuals with low CD4/CD8 ratio despite effective antiretroviral therapy exhibit altered T cell subsets, heightened CD8+ T cell activation, and increased risk of non-AIDS morbidity and mortality.PLoS Pathog. 2014 May 15;10(5):e1004078. doi: 10.1371/journal.ppat.1004078. eCollection 2014 May. PLoS Pathog. 2014. PMID: 24831517 Free PMC article. Clinical Trial.
-
T-Cell Activation Independently Associates With Immune Senescence in HIV-Infected Recipients of Long-term Antiretroviral Treatment.J Infect Dis. 2016 Jul 15;214(2):216-25. doi: 10.1093/infdis/jiw146. Epub 2016 Apr 12. J Infect Dis. 2016. PMID: 27073222 Free PMC article.
-
Residual immune dysregulation syndrome in treated HIV infection.Adv Immunol. 2013;119:51-83. doi: 10.1016/B978-0-12-407707-2.00002-3. Adv Immunol. 2013. PMID: 23886064 Free PMC article. Review.
-
Gut epithelial barrier dysfunction in human immunodeficiency virus-hepatitis C virus coinfected patients: Influence on innate and acquired immunity.World J Gastroenterol. 2016 Jan 28;22(4):1433-48. doi: 10.3748/wjg.v22.i4.1433. World J Gastroenterol. 2016. PMID: 26819512 Free PMC article. Review.
Cited by
-
Cardiovascular Disease, Statins, and HIV.J Infect Dis. 2016 Oct 1;214 Suppl 2(Suppl 2):S83-92. doi: 10.1093/infdis/jiw288. J Infect Dis. 2016. PMID: 27625435 Free PMC article. Review.
-
Abnormal Levels of Some Biomarkers of Immune Activation Despite Very Early Treatment of Human Immunodeficiency Virus.J Infect Dis. 2021 May 20;223(9):1621-1630. doi: 10.1093/infdis/jiaa580. J Infect Dis. 2021. PMID: 32915986 Free PMC article.
-
Cardiovascular Disease and Thrombosis in HIV Infection.Arterioscler Thromb Vasc Biol. 2023 Feb;43(2):175-191. doi: 10.1161/ATVBAHA.122.318232. Epub 2022 Dec 1. Arterioscler Thromb Vasc Biol. 2023. PMID: 36453273 Free PMC article. Review.
-
Identification of Immune Activation Profiles That May Predict Morbidity During Antiretroviral Therapy Treated HIV Infection.EBioMedicine. 2016 Jun;8:16-17. doi: 10.1016/j.ebiom.2016.05.012. Epub 2016 May 13. EBioMedicine. 2016. PMID: 27428408 Free PMC article. No abstract available.
-
The microbiota as a modulator of mucosal inflammation and HIV/HPV pathogenesis: From association to causation.Front Immunol. 2023 Jan 23;14:1072655. doi: 10.3389/fimmu.2023.1072655. eCollection 2023. Front Immunol. 2023. PMID: 36756132 Free PMC article. Review.
References
-
- Lohse N, Hansen AB, Pedersen G, et al. Survival of persons with and without HIV infection in Denmark, 1995–2005. Ann Intern Med. 2007;146:87–95. - PubMed
-
- van Sighem AI, Gras LA, Reiss P, Brinkman K, de Wolf F. Life expectancy of recently diagnosed asymptomatic HIV-infected patients approaches that of uninfected individuals. AIDS. 2010;24:1527–35. - PubMed
-
- Lewden C, Bouteloup V, De Wit S, et al. All-cause mortality in treated HIV-infected adults with CD4 >/=500/mm3 compared with the general population: evidence from a large European observational cohort collaboration. Int J Epidemiol. 2012;41:433–45. - PubMed
Publication types
MeSH terms
Grants and funding
- P30 MH062246/MH/NIMH NIH HHS/United States
- P01AI076174/AI/NIAID NIH HHS/United States
- R00 HL108743/HL/NHLBI NIH HHS/United States
- K24AI069994/AI/NIAID NIH HHS/United States
- R56AI100765/AI/NIAID NIH HHS/United States
- K24 AI069994/AI/NIAID NIH HHS/United States
- U10EY008052/EY/NEI NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- R21 AI087035/AI/NIAID NIH HHS/United States
- R01 AI087145/AI/NIAID NIH HHS/United States
- U10 EY008057/EY/NEI NIH HHS/United States
- U10 EY008052/EY/NEI NIH HHS/United States
- UL1RR024131/RR/NCRR NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- R24AI067039/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- P01 AI076174/AI/NIAID NIH HHS/United States
- P30MH62246/MH/NIMH NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- 1K99HL108743/HL/NHLBI NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- R56 AI100765/AI/NIAID NIH HHS/United States
- U10EY008067/EY/NEI NIH HHS/United States
- U10 EY008067/EY/NEI NIH HHS/United States
- U10EY008057/EY/NEI NIH HHS/United States
- K99 HL108743/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
