

Early clearance of Mycobacterium tuberculosis: a new frontier in prevention
- PMID: 24754048
- PMCID: PMC3956425
- DOI: 10.1111/imm.12223
Early clearance of Mycobacterium tuberculosis: a new frontier in prevention
Abstract
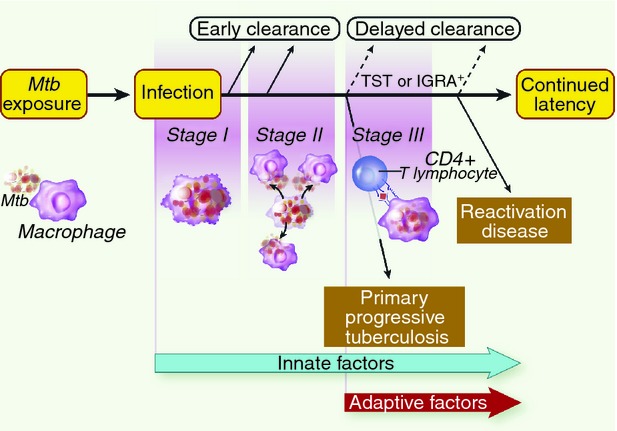
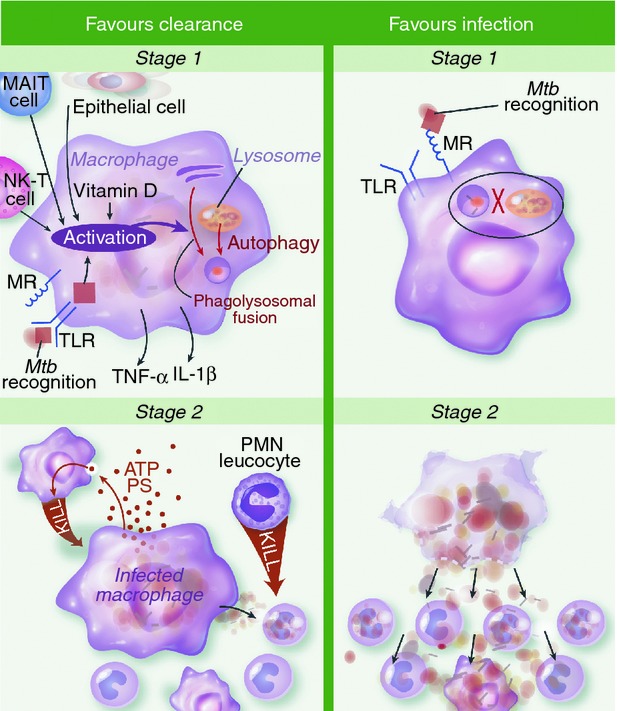
Early clearance (EC) is the successful eradication of inhaled Mycobacterium tuberculosis before an adaptive immune response develops. Evidence for EC comes from case contact studies that consistently show that a proportion of heavily exposed individuals do not develop M. tuberculosis infection. Further support for the existence of this phenotype comes from genetic loci associated with tuberculin reactivity. In this review we discuss aspects of the innate response that may underpin EC and hypotheses that can be tested through field laboratory link studies in M. tuberculosis case contacts. Specifically, we consider mechanisms whereby alveolar macrophages recognize and kill intracellular M. tuberculosis, and how other cell types, such as neutrophils, natural killer T cells, mucosa-associated invariant T cells and cd T cells may assist. How EC may be impaired by HIV infection or vitamin D deficiency is also explored. As EC is a form of protective immunity, further study may advance the development of vaccines and immunotherapies to prevent M. tuberculosis infection.
© 2013 John Wiley & Sons Ltd.
Figures
Similar articles
-
T cells and adaptive immunity to Mycobacterium tuberculosis in humans.Immunol Rev. 2015 Mar;264(1):74-87. doi: 10.1111/imr.12274. Immunol Rev. 2015. PMID: 25703553 Review.
-
HIV-1 Infection Is Associated with Depletion and Functional Impairment of Mycobacterium tuberculosis-Specific CD4 T Cells in Individuals with Latent Tuberculosis Infection.J Immunol. 2017 Sep 15;199(6):2069-2080. doi: 10.4049/jimmunol.1700558. Epub 2017 Jul 31. J Immunol. 2017. PMID: 28760884 Free PMC article.
-
HIV and the tuberculosis "set point": how HIV impairs alveolar macrophage responses to tuberculosis and sets the stage for progressive disease.Retrovirology. 2020 Sep 23;17(1):32. doi: 10.1186/s12977-020-00540-2. Retrovirology. 2020. PMID: 32967690 Free PMC article. Review.
-
Mycobacterium tuberculosis Primary Infection and Dissemination: A Critical Role for Alveolar Epithelial Cells.Front Cell Infect Microbiol. 2019 Aug 21;9:299. doi: 10.3389/fcimb.2019.00299. eCollection 2019. Front Cell Infect Microbiol. 2019. PMID: 31497538 Free PMC article. Review.
-
Impaired Recognition of Mycobacterium tuberculosis by Alveolar Macrophages From Diabetic Mice.J Infect Dis. 2016 Dec 1;214(11):1629-1637. doi: 10.1093/infdis/jiw436. Epub 2016 Sep 13. J Infect Dis. 2016. PMID: 27630197 Free PMC article.
Cited by
-
Mycobacterial Regulatory Systems Involved in the Regulation of Gene Expression Under Respiration-Inhibitory Conditions.J Microbiol. 2023 Mar;61(3):297-315. doi: 10.1007/s12275-023-00026-8. Epub 2023 Feb 27. J Microbiol. 2023. PMID: 36847970 Review.
-
Immune stability predicts tuberculosis infection risk in a wild mammal.Proc Biol Sci. 2019 Oct 9;286(1912):20191401. doi: 10.1098/rspb.2019.1401. Epub 2019 Oct 2. Proc Biol Sci. 2019. PMID: 31575363 Free PMC article.
-
Polymorphisms in CARD8 and NLRP3 are associated with extrapulmonary TB and poor clinical outcome in active TB in Ethiopia.Sci Rep. 2019 Feb 28;9(1):3126. doi: 10.1038/s41598-019-40121-8. Sci Rep. 2019. PMID: 30816317 Free PMC article.
-
Concomitant disseminated histoplasmosis and disseminated tuberculosis after tumor necrosis factor inhibitor treatment: a case report.BMC Infect Dis. 2017 Jan 13;17(1):70. doi: 10.1186/s12879-016-2097-7. BMC Infect Dis. 2017. PMID: 28086756 Free PMC article.
-
Trained immunity contributes to the prevention of Mycobacterium tuberculosis infection, a novel role of autophagy.Emerg Microbes Infect. 2021 Dec;10(1):578-588. doi: 10.1080/22221751.2021.1899771. Emerg Microbes Infect. 2021. PMID: 33666534 Free PMC article. Review.
References
-
- WHO. Geneva: World Health Organization; http://www.who.int/mediacentre/factsheets/fs104/en/ [accessed on 12 March 2013]Tuberculosis [Internet]WHO Available from:
-
- Brennan MJ, Thole J. Tuberculosis vaccines: a strategic blueprint for the next decade. Tuberculosis (Edinb) 2012;92(Suppl. 1):S6–13. - PubMed
-
- Israel HL, Hetherington HW, Ord JG. A study of tuberculosis among students of nursing. JAMA. 1941;117:839–44.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
