

Comparison of liver fat indices for the diagnosis of hepatic steatosis and insulin resistance
- PMID: 24732091
- PMCID: PMC3986069
- DOI: 10.1371/journal.pone.0094059
Comparison of liver fat indices for the diagnosis of hepatic steatosis and insulin resistance
Abstract
Context: Hepatic steatosis, defined as increased hepatocellular lipid content (HCL), associates with visceral obesity and glucose intolerance. As exact HCL quantification by 1H-magnetic resonance spectroscopy (1H-MRS) is not generally available, various clinical indices are increasingly used to predict steatosis.
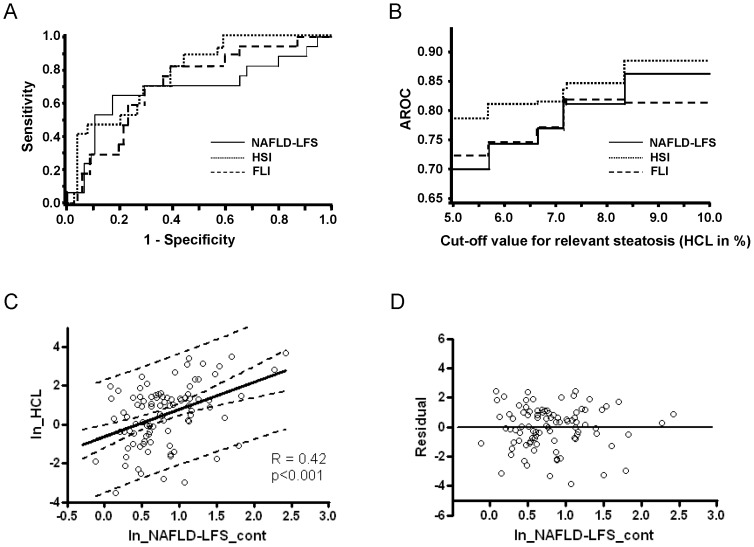
Objective: The purpose of this study was to test the accuracy of NAFLD liver fat score (NAFLD-LFS), hepatic steatosis index (HSI) and fatty liver index (FLI) against 1H-MRS and their relationships with insulin sensitivity and secretion.
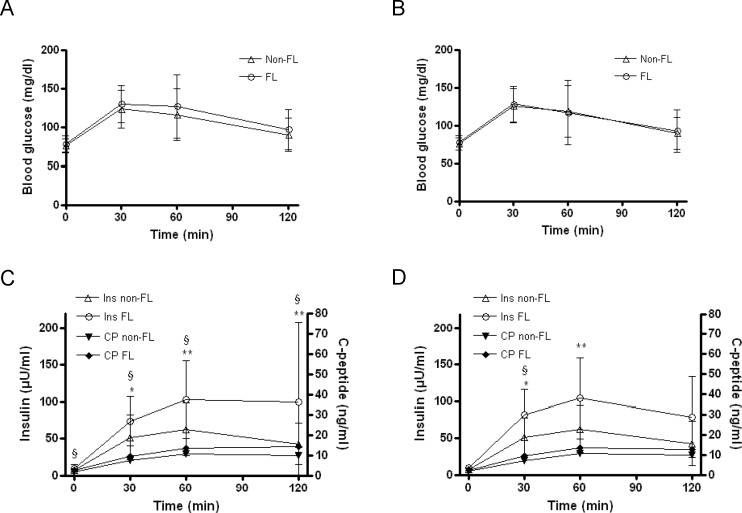
Design, setting and participants: Ninety-two non-diabetic, predominantly non-obese humans underwent clinical examination, 1H-MRS and an oral glucose tolerance test (OGTT) to calculate insulin sensitivity and β-cell function. Accuracy of indices was assessed from the area under the receiver operating characteristic curve (AROC).
Results: Median HCL was 2.49% (0.62;4.23) and correlated with parameters of glycemia across all subjects. NAFLD-LFS, FLI and HSI yielded AROCs of 0.70, 0.72, and 0.79, respectively, and related positively to HCL, insulin resistance, fasting and post-load β-cell function normalized for insulin resistance. Upon adjustment for age, sex and HCL, regression analysis revealed that NAFLD-LFS, FLI and HSI still independently associated with both insulin sensitivity and β-cell function.
Conclusion: The tested indices offer modest efficacy to detect steatosis and cannot substitute for fat quantification by 1H-MRS. However, all indices might serve as surrogate parameters for liver fat content and also as rough clinical estimates of abnormal insulin sensitivity and secretion. Further validation in larger collectives such as epidemiological studies is needed.
Conflict of interest statement
Figures
Similar articles
-
Liver Fat Scores for Noninvasive Diagnosis and Monitoring of Nonalcoholic Fatty Liver Disease in Epidemiological and Clinical Studies.J Clin Transl Hepatol. 2023 Oct 28;11(5):1212-1227. doi: 10.14218/JCTH.2022.00019. Epub 2023 May 31. J Clin Transl Hepatol. 2023. PMID: 37577225 Free PMC article. Review.
-
External validation of the fatty liver index and lipid accumulation product indices, using 1H-magnetic resonance spectroscopy, to identify hepatic steatosis in healthy controls and obese, insulin-resistant individuals.Eur J Endocrinol. 2014 Nov;171(5):561-9. doi: 10.1530/EJE-14-0112. Eur J Endocrinol. 2014. PMID: 25298375
-
Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease.Aliment Pharmacol Ther. 2014 Nov;40(10):1209-22. doi: 10.1111/apt.12963. Epub 2014 Sep 29. Aliment Pharmacol Ther. 2014. PMID: 25267215
-
Intact Fasting Insulin Identifies Nonalcoholic Fatty Liver Disease in Patients Without Diabetes.J Clin Endocrinol Metab. 2021 Oct 21;106(11):e4360-e4371. doi: 10.1210/clinem/dgab417. J Clin Endocrinol Metab. 2021. PMID: 34190318
-
Comparative analysis of the relationship between four hepatic steatosis indices and muscle mass.Sci Rep. 2023 Jan 30;13(1):1645. doi: 10.1038/s41598-023-28751-5. Sci Rep. 2023. PMID: 36717652 Free PMC article. Review.
Cited by
-
Significance of single and multi-voxel 1H magnetic resonance spectroscopy in the quantification of myocellular lipid in young non-obese Asian Indian males.Magn Reson Imaging. 2021 Jan;75:65-71. doi: 10.1016/j.mri.2020.07.011. Epub 2020 Jul 28. Magn Reson Imaging. 2021. PMID: 32735818 Free PMC article.
-
Liver fat scores do not reflect interventional changes in liver fat content induced by high-protein diets.Sci Rep. 2021 Apr 23;11(1):8843. doi: 10.1038/s41598-021-87360-2. Sci Rep. 2021. PMID: 33893355 Free PMC article. Clinical Trial.
-
Nonalcoholic fatty liver disease and type 2 diabetes: common pathophysiologic mechanisms.Curr Diab Rep. 2015 Jun;15(6):607. doi: 10.1007/s11892-015-0607-4. Curr Diab Rep. 2015. PMID: 25894944 Review.
-
Liver Fat Scores for Noninvasive Diagnosis and Monitoring of Nonalcoholic Fatty Liver Disease in Epidemiological and Clinical Studies.J Clin Transl Hepatol. 2023 Oct 28;11(5):1212-1227. doi: 10.14218/JCTH.2022.00019. Epub 2023 May 31. J Clin Transl Hepatol. 2023. PMID: 37577225 Free PMC article. Review.
-
Ultrasound elastography in patients with fatty liver disease.Radiol Bras. 2020 Jan-Feb;53(1):47-55. doi: 10.1590/0100-3984.2019.0028. Radiol Bras. 2020. PMID: 32313337 Free PMC article. Review.
References
-
- Roden M (2006) Mechanisms of Disease: hepatic steatosis in type 2 diabetes–pathogenesis and clinical relevance. Nat Clin Pract Endocrinol Metab 2: 335–348. - PubMed
-
- Webb M, Yeshua H, Zelber-Sagi S, Santo E, Brazowski E, et al. (2009) Diagnostic value of a computerized hepatorenal index for sonographic quantification of liver steatosis. AJR Am J Roentgenol 192: 909–914. - PubMed
-
- Lee JH, Kim D, Kim HJ, Lee CH, Yang JI, et al. (2010) Hepatic steatosis index: a simple screening tool reflecting nonalcoholic fatty liver disease. Dig Liver Dis 42: 503–508. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
