

Cytomegalovirus viral load kinetics in patients with HIV/AIDS admitted to a medical intensive care unit: a case for pre-emptive therapy
- PMID: 24699683
- PMCID: PMC3974798
- DOI: 10.1371/journal.pone.0093702
Cytomegalovirus viral load kinetics in patients with HIV/AIDS admitted to a medical intensive care unit: a case for pre-emptive therapy
Abstract
Background: Cytomegalovirus (CMV) infection is associated with severe diseases in immunosuppressed patients; however, there is a lack of data for pre-emptive therapy in patients with HIV/AIDS.
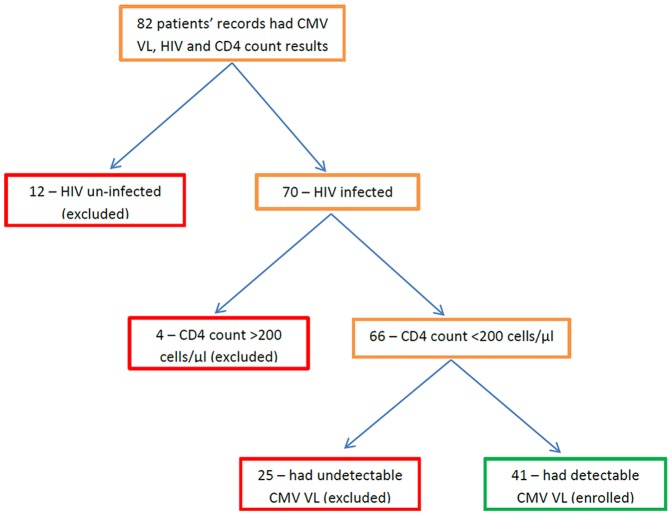
Method: This was a retrospective study, which enrolled patients diagnosed with HIV/AIDS (CD4<200 cells/μl), who had detectable CMV viral load (VL) during their stay in an adult medical intensive care unit between 2009-2012.
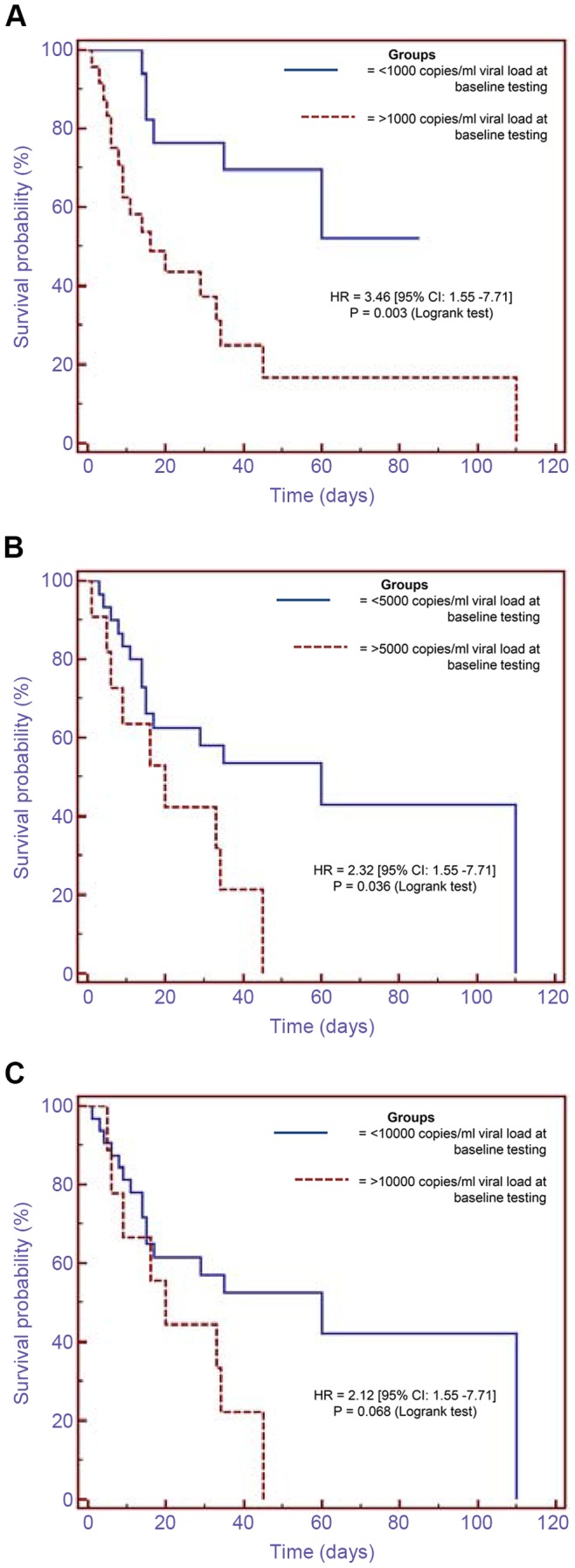
Results: After screening 82 patients' records, 41 patients met the enrolment criteria. Their median age was 37 (interquartile range [IQR]: 31-46), and median CD4 count was 29 cells/μl (IQR: 5-55). Sixteen patients (39%) had serial measurements of CMV VL before treatment with ganciclovir. Patients whose baseline CMV VL values were between 1,000-3,000 copies/ml had significantly higher values (median of 14,650 copies/ml) on follow-up testing done 4-12 days later. Those with undetectable VLs at baseline testing had detectable VLs (median of 1,590 copies/ml) mostly within 20 days of follow-up testing. Patients who had VLs >1,000 copies/ml at baseline testing had significantly higher mortality compared to those who had <1,000 copies/ml {hazard ratio of 3.46, p = 0.003 [95% confidence interval (CI): 1.55-7.71]}. Analysis of the highest CMV VL per patient showed that patients who had VLs of >5,100 copies/ml and did not receive ganciclovir had 100% mortality compared to 58% mortality in those who received ganciclovir at VLs of >5,100 copies/ml, 50% mortality in those who were not treated and had low VLs of <5,100 copies/ml, and 44% mortality in those who had ganciclovir treatment at VLs of <5,100 copies/ml (p = 0.084, 0.046, 0.037, respectively).
Conclusion: This study showed a significantly increased mortality in patients with HIV/AIDS who had high CMV VLs, and suggests that a threshold value of 1,000 copies/ml may be appropriate for pre-emptive treatment in this group.
Conflict of interest statement
Figures
Similar articles
-
Assessment of the efficacy and safety of pre-emptive anti-cytomegalovirus (CMV) therapy in HIV-infected patients with CMV viraemia.Int J STD AIDS. 2015 Apr;26(5):306-12. doi: 10.1177/0956462414536146. Epub 2014 May 20. Int J STD AIDS. 2015. PMID: 24845948
-
Impact of CMV therapy with valganciclovir on immune activation and the HIV viral load in semen and blood: an observational clinical study.J Acquir Immune Defic Syndr. 2014 Mar 1;65(3):251-8. doi: 10.1097/01.qai.0000435256.34306.c1. J Acquir Immune Defic Syndr. 2014. PMID: 24091693
-
Management of allogeneic bone marrow transplant recipients at risk for cytomegalovirus disease using a surveillance bronchoscopy and prolonged pre-emptive ganciclovir therapy.J Clin Virol. 1999 Aug;13(3):149-59. doi: 10.1016/s1386-6532(99)00029-3. J Clin Virol. 1999. PMID: 10443791 Clinical Trial.
-
Oral valganciclovir versus ganciclovir as delayed pre-emptive therapy for patients after allogeneic hematopoietic stem cell transplant: a pilot trial (04-0274) and review of the literature.Transpl Infect Dis. 2012 Jun;14(3):259-67. doi: 10.1111/j.1399-3062.2011.00689.x. Epub 2011 Oct 28. Transpl Infect Dis. 2012. PMID: 22093134 Review.
-
Current management strategies for the prevention and treatment of cytomegalovirus infection in pediatric transplant recipients.Paediatr Drugs. 2002;4(5):279-90. doi: 10.2165/00128072-200204050-00001. Paediatr Drugs. 2002. PMID: 11994033 Review.
Cited by
-
Characteristics and outcomes of patients admitted to a tertiary academic hospital in Pretoria with HIV and severe pneumonia: a retrospective cohort study.BMC Infect Dis. 2022 Jun 15;22(1):548. doi: 10.1186/s12879-022-07522-z. BMC Infect Dis. 2022. PMID: 35705920 Free PMC article.
-
Predictors of in-hospital mortality in a cohort of people living with HIV (PLHIV) admitted to an academic medical intensive care unit from 2009 to 2014: A retrospective cohort study.Medicine (Baltimore). 2022 Jul 15;101(28):e29750. doi: 10.1097/MD.0000000000029750. Medicine (Baltimore). 2022. PMID: 35839058 Free PMC article.
-
Ongoing burden of disease and mortality from HIV/CMV coinfection in Africa in the antiretroviral therapy era.Front Microbiol. 2015 Sep 24;6:1016. doi: 10.3389/fmicb.2015.01016. eCollection 2015. Front Microbiol. 2015. PMID: 26441939 Free PMC article. Review.
-
Human cytomegalovirus (CMV) in Africa: a neglected but important pathogen.J Virus Erad. 2016 Jul 1;2(3):136-42. doi: 10.1016/S2055-6640(20)30456-8. J Virus Erad. 2016. PMID: 27482452 Free PMC article.
-
Comparison of Two Commercial Automated Nucleic Acid Extraction and Integrated Quantitation Real-Time PCR Platforms for the Detection of Cytomegalovirus in Plasma.PLoS One. 2016 Aug 5;11(8):e0160493. doi: 10.1371/journal.pone.0160493. eCollection 2016. PLoS One. 2016. PMID: 27494707 Free PMC article.
References
-
- Atkinson C, Emery VC (2011) Cytomegalovirus quantification: Where to next in optimising patient management? J Clin Virol 51: 223–8. - PubMed
-
- Sundar IK (2004) Update: cytomegalovirus infection in HIV-infected patients – a review. Clin Microbiol Newsl 26: 137–44.
-
- Mocarski Jr ES, Shenk T, Pass RF (2007) Cytomegaloviruses. In: Knipe DM, Howley PM, Griffin DE, Lamb RA, Martin MA, Roizman B, et al.., editors. Fields Virology. 5th ed. Philadelphia: Lippincot Williams & Wilkins, a Wolters Kluwer business. pp. 2701–72.
-
- Barron MA, Weinberg A (2005) Common viral infections in transplant recipients, part 1. Herpesviruses. Clin Microbiol Newsl 27: 99–106.
-
- De la Hoz RE, Stephens G, Sherlock C (2002) Diagnosis and treatment approaches of CMV infections in adult patients. J Clin Virol 25: 1–12. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
