

Validity of myocardial infarction diagnoses in administrative databases: a systematic review
- PMID: 24682186
- PMCID: PMC3969323
- DOI: 10.1371/journal.pone.0092286
Validity of myocardial infarction diagnoses in administrative databases: a systematic review
Abstract
Background: Though administrative databases are increasingly being used for research related to myocardial infarction (MI), the validity of MI diagnoses in these databases has never been synthesized on a large scale.
Objective: To conduct the first systematic review of studies reporting on the validity of diagnostic codes for identifying MI in administrative data.
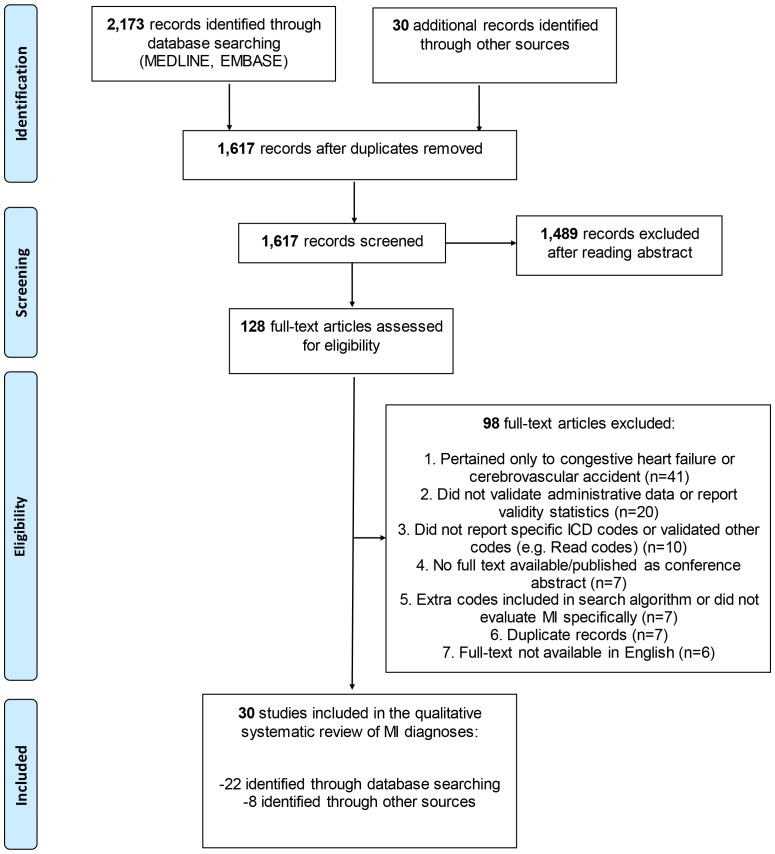
Methods: MEDLINE and EMBASE were searched (inception to November 2010) for studies: (a) Using administrative data to identify MI; or (b) Evaluating the validity of MI codes in administrative data; and (c) Reporting validation statistics (sensitivity, specificity, positive predictive value (PPV), negative predictive value, or Kappa scores) for MI, or data sufficient for their calculation. Additonal articles were located by handsearch (up to February 2011) of original papers. Data were extracted by two independent reviewers; article quality was assessed using the Quality Assessment of Diagnostic Accuracy Studies tool.
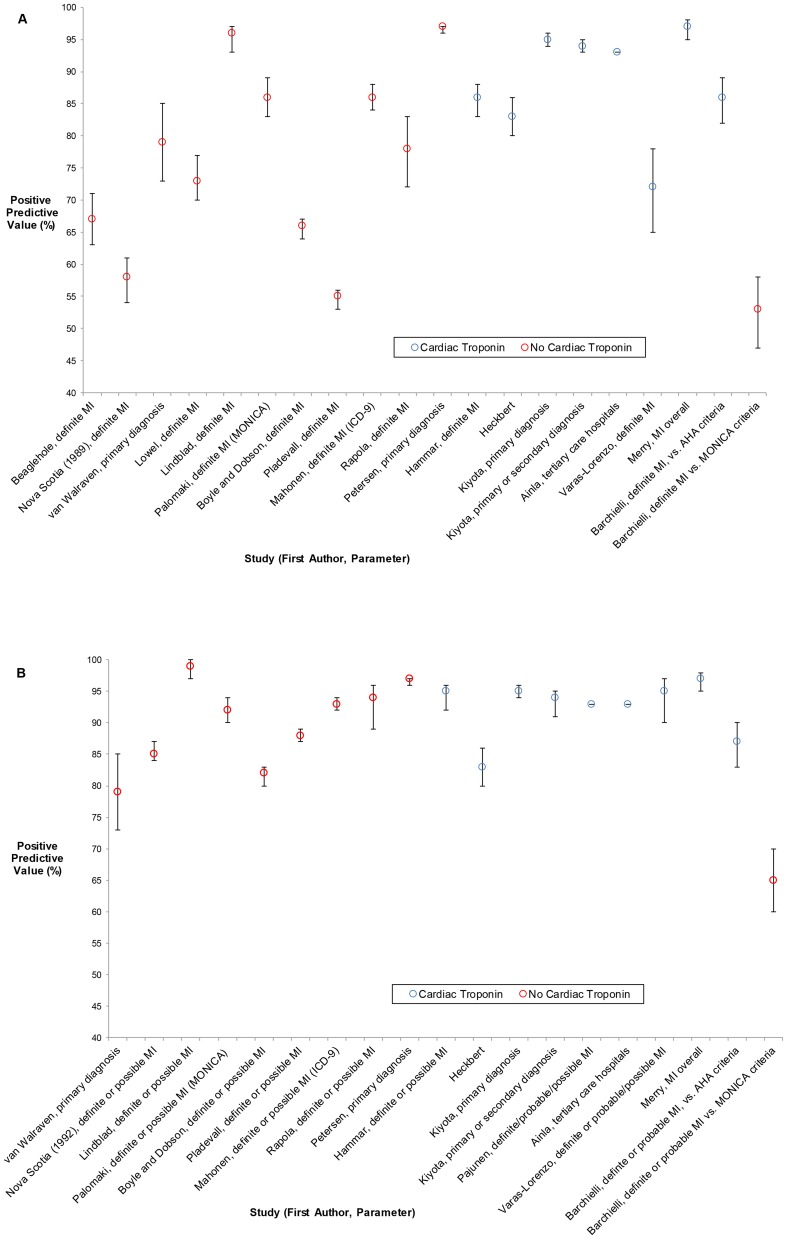
Results: Thirty studies published from 1984-2010 were included; most assessed codes from the International Classification of Diseases (ICD)-9th revision. Sensitivity and specificity of hospitalization data for identifying MI in most [≥50%] studies was ≥86%, and PPV in most studies was ≥93%. The PPV was higher in the more-recent studies, and lower when criteria that do not incorporate cardiac troponin levels (such as the MONICA) were employed as the gold standard. MI as a cause-of-death on death certificates also demonstrated lower accuracy, with maximum PPV of 60% (for definite MI).
Conclusions: Hospitalization data has higher validity and hence can be used to identify MI, but the accuracy of MI as a cause-of-death on death certificates is suboptimal, and more studies are needed on the validity of ICD-10 codes. When using administrative data for research purposes, authors should recognize these factors and avoid using vital statistics data if hospitalization data is not available to confirm deaths from MI.
Conflict of interest statement
Figures
Similar articles
-
Validity of Diagnostic Codes for Acute Stroke in Administrative Databases: A Systematic Review.PLoS One. 2015 Aug 20;10(8):e0135834. doi: 10.1371/journal.pone.0135834. eCollection 2015. PLoS One. 2015. PMID: 26292280 Free PMC article.
-
Validity of heart failure diagnoses in administrative databases: a systematic review and meta-analysis.PLoS One. 2014 Aug 15;9(8):e104519. doi: 10.1371/journal.pone.0104519. eCollection 2014. PLoS One. 2014. PMID: 25126761 Free PMC article. Review.
-
Diagnostic Algorithms for Cardiovascular Death in Administrative Claims Databases: A Systematic Review.Drug Saf. 2019 Apr;42(4):515-527. doi: 10.1007/s40264-018-0754-z. Drug Saf. 2019. PMID: 30471046
-
Chart validation of inpatient ICD-9-CM administrative diagnosis codes for acute myocardial infarction (AMI) among intravenous immune globulin (IGIV) users in the Sentinel Distributed Database.Pharmacoepidemiol Drug Saf. 2018 Apr;27(4):398-404. doi: 10.1002/pds.4398. Epub 2018 Feb 15. Pharmacoepidemiol Drug Saf. 2018. PMID: 29446185 Free PMC article.
-
A systematic review of validated methods for identifying patients with rheumatoid arthritis using administrative or claims data.Vaccine. 2013 Dec 30;31 Suppl 10:K41-61. doi: 10.1016/j.vaccine.2013.03.075. Vaccine. 2013. PMID: 24331074 Review.
Cited by
-
Optimal threshold of adherence to lipid lowering drugs in predicting acute coronary syndrome, stroke, or mortality: A cohort study.PLoS One. 2019 Sep 25;14(9):e0223062. doi: 10.1371/journal.pone.0223062. eCollection 2019. PLoS One. 2019. PMID: 31553787 Free PMC article.
-
Existing comorbidities in people with osteoarthritis: a retrospective analysis of a population-based cohort in Alberta, Canada.BMJ Open. 2019 Nov 21;9(11):e033334. doi: 10.1136/bmjopen-2019-033334. BMJ Open. 2019. PMID: 31753902 Free PMC article.
-
Psychostimulants/Atomoxetine and Serious Cardiovascular Events in Children with ADHD or Autism Spectrum Disorder.CNS Drugs. 2020 Jan;34(1):93-101. doi: 10.1007/s40263-019-00686-4. CNS Drugs. 2020. PMID: 31768949 Free PMC article.
-
Twenty-Year Trends in Outcomes for Older Adults With Acute Myocardial Infarction in the United States.JAMA Netw Open. 2019 Mar 1;2(3):e191938. doi: 10.1001/jamanetworkopen.2019.1938. JAMA Netw Open. 2019. PMID: 30874787 Free PMC article.
-
Established evidence-based treatment guidelines help mitigate disparities in quality of emergency care.Acad Emerg Med. 2021 Sep;28(9):1051-1060. doi: 10.1111/acem.14235. Epub 2021 Jun 28. Acad Emerg Med. 2021. PMID: 33599040 Free PMC article.
References
-
- Health statistics and informatics department, World Health Organization (2011) Causes of Death 2008 Summary Tables. Available: http://www.who.int/healthinfo/global_burden_disease/estimates_regional_2.... Accessed 2014 March 10.
-
- Leal J, Luengo-Fernandez R, Gray A, Petersen S, Rayner M (2006) Economic burden of cardiovascular diseases in the enlarged European Union. Eur Heart J 27: 1610–1619. - PubMed
-
- Mensah GA, Brown DW (2007) An overview of cardiovascular disease burden in the United States. Health Aff (Millwood) 26: 38–48. - PubMed
-
- Gonzalez A, Maradit Kremers H, Crowson CS, Ballman KV, Roger VL, et al. (2008) Do cardiovascular risk factors confer the same risk for cardiovascular outcomes in rheumatoid arthritis patients as in non-rheumatoid arthritis patients? Ann Rheum Dis 67: 64–69. - PubMed
-
- Kuo CF, Yu KH, See LC, Chou IJ, Ko YS, et al. (2013) Risk of myocardial infarction among patients with gout: a nationwide population-based study. Rheumatology (Oxford) 52: 111–117. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
