

Epidemiological analysis, detection, and comparison of space-time patterns of Beijing hand-foot-mouth disease (2008-2012)
- PMID: 24663329
- PMCID: PMC3963949
- DOI: 10.1371/journal.pone.0092745
Epidemiological analysis, detection, and comparison of space-time patterns of Beijing hand-foot-mouth disease (2008-2012)
Abstract
Background: Hand, foot, and mouth disease (HFMD) mostly affects the health of infants and preschool children. Many studies of HFMD in different regions have been published. However, the epidemiological characteristics and space-time patterns of individual-level HFMD cases in a major city such as Beijing are unknown. The objective of this study was to investigate epidemiological features and identify high relative risk space-time HFMD clusters at a fine spatial scale.
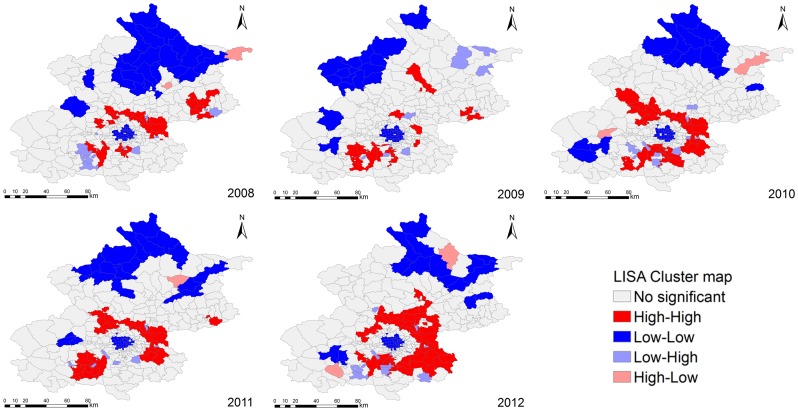
Methods: Detailed information on age, occupation, pathogen and gender was used to analyze the epidemiological features of HFMD epidemics. Data on individual-level HFMD cases were examined using Local Indicators of Spatial Association (LISA) analysis to identify the spatial autocorrelation of HFMD incidence. Spatial filtering combined with scan statistics methods were used to detect HFMD clusters.
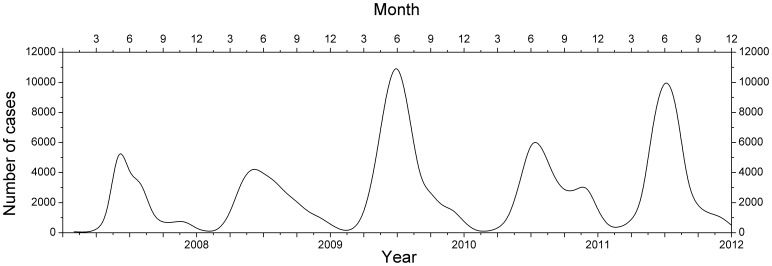
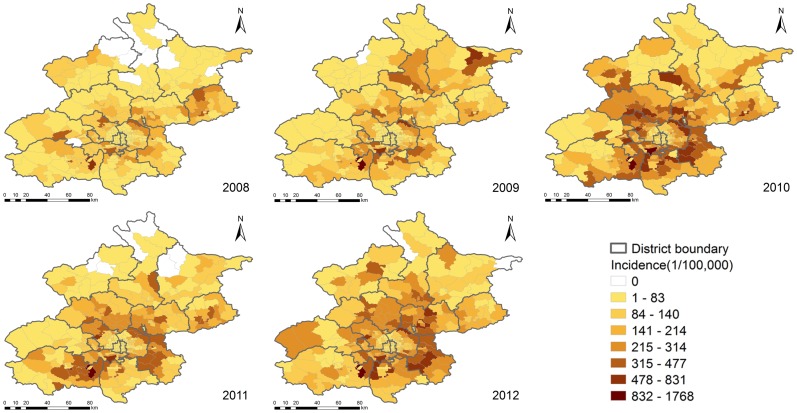
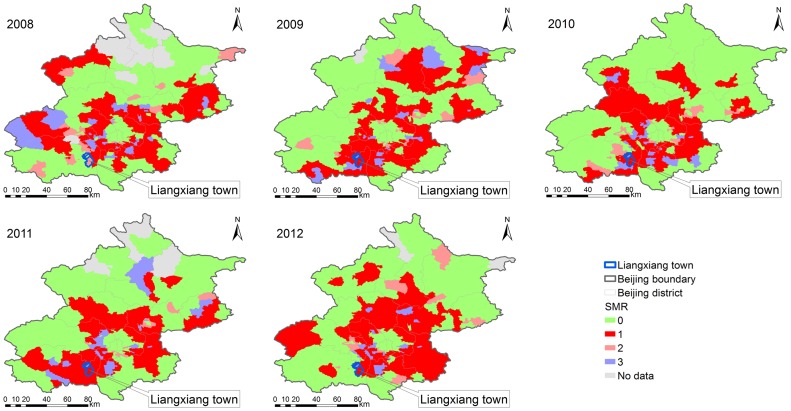
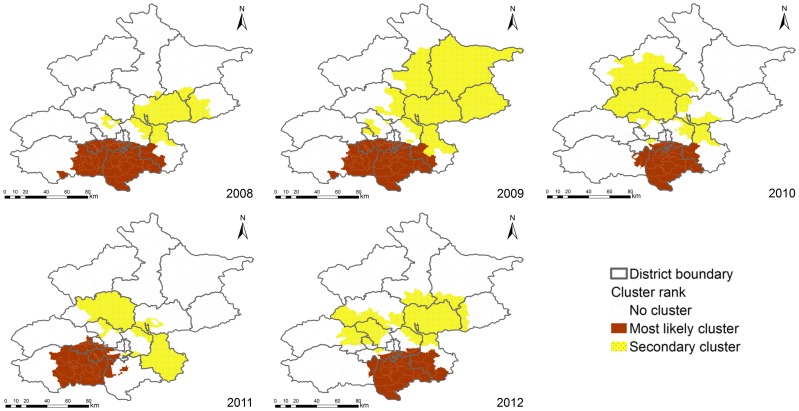
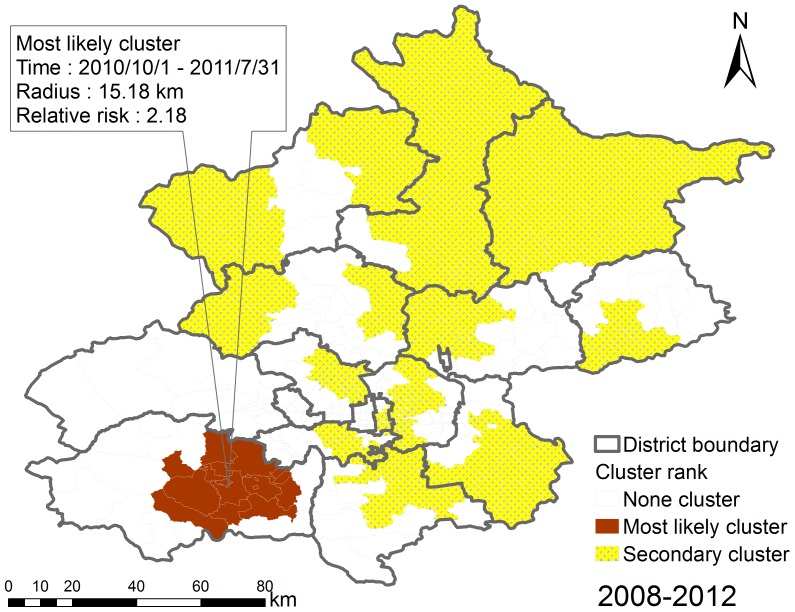
Results: A total of 157,707 HFMD cases (60.25% were male, 39.75% were female) reported in Beijing from 2008 to 2012 included 1465 severe cases and 33 fatal cases. The annual average incidence rate was 164.3 per 100,000 (ranged from 104.2 in 2008 to 231.5 in 2010). Male incidence was higher than female incidence for the 0 to 14-year age group, and 93.88% were nursery children or lived at home. Areas at a higher relative risk were mainly located in the urban-rural transition zones (the percentage of the population at risk ranged from 33.89% in 2011 to 39.58% in 2012) showing High-High positive spatial association for HFMD incidence. The most likely space-time cluster was located in the mid-east part of the Fangshan district, southwest of Beijing.
Conclusions: The spatial-time patterns of Beijing HFMD (2008-2012) showed relatively steady. The population at risk were mainly distributed in the urban-rural transition zones. Epidemiological features of Beijing HFMD were generally consistent with the previous research. The findings generated computational insights useful for disease surveillance, risk assessment and early warning.
Conflict of interest statement
Figures

Similar articles
-
Epidemiological Characteristics and Spatial-Temporal Clusters of Hand, Foot, and Mouth Disease in Zhejiang Province, China, 2008-2012.PLoS One. 2015 Sep 30;10(9):e0139109. doi: 10.1371/journal.pone.0139109. eCollection 2015. PLoS One. 2015. PMID: 26422015 Free PMC article.
-
Detecting spatial-temporal cluster of hand foot and mouth disease in Beijing, China, 2009-2014.BMC Infect Dis. 2016 May 17;16:206. doi: 10.1186/s12879-016-1547-6. BMC Infect Dis. 2016. PMID: 27184561 Free PMC article.
-
Epidemiological characteristics and spatial-temporal clusters of hand, foot, and mouth disease in Qingdao City, China, 2013-2018.PLoS One. 2020 Jun 5;15(6):e0233914. doi: 10.1371/journal.pone.0233914. eCollection 2020. PLoS One. 2020. PMID: 32502174 Free PMC article.
-
Spatio-temporal analysis of the relationship between meteorological factors and hand-foot-mouth disease in Beijing, China.BMC Infect Dis. 2018 Apr 3;18(1):158. doi: 10.1186/s12879-018-3071-3. BMC Infect Dis. 2018. PMID: 29614964 Free PMC article.
-
Epidemiological characteristics and temporal-spatial clustering analysis of hand, foot and mouth disease in Nanchang city 2008-2012.Infect Dis (Lond). 2015 Jan;47(1):33-8. doi: 10.3109/00365548.2014.964762. Epub 2014 Nov 17. Infect Dis (Lond). 2015. PMID: 25400030
Cited by
-
Epidemiological Characteristics and Spatial-Temporal Clusters of Hand, Foot, and Mouth Disease in Zhejiang Province, China, 2008-2012.PLoS One. 2015 Sep 30;10(9):e0139109. doi: 10.1371/journal.pone.0139109. eCollection 2015. PLoS One. 2015. PMID: 26422015 Free PMC article.
-
Age patterns and transmission characteristics of hand, foot and mouth disease in China.BMC Infect Dis. 2016 Nov 21;16(1):691. doi: 10.1186/s12879-016-2008-y. BMC Infect Dis. 2016. PMID: 27871252 Free PMC article.
-
The effect of meteorological variables on the transmission of hand, foot and mouth disease in four major cities of shanxi province, China: a time series data analysis (2009-2013).PLoS Negl Trop Dis. 2015 Mar 5;9(3):e0003572. doi: 10.1371/journal.pntd.0003572. eCollection 2015 Mar. PLoS Negl Trop Dis. 2015. PMID: 25742504 Free PMC article.
-
Determinants of the Transmission Variation of Hand, Foot and Mouth Disease in China.PLoS One. 2016 Oct 4;11(10):e0163789. doi: 10.1371/journal.pone.0163789. eCollection 2016. PLoS One. 2016. PMID: 27701445 Free PMC article.
-
The impact of hand, foot and mouth disease control policies in Singapore: A qualitative analysis of public perceptions.J Public Health Policy. 2017 May;38(2):271-287. doi: 10.1057/s41271-017-0066-z. J Public Health Policy. 2017. PMID: 28533530 Free PMC article.
References
-
- Ni H, Yi B, Yin J, Fang T, He T, et al. (2012) Epidemiological and etiological characteristics of hand, foot, and mouth disease in Ningbo, China, 2008–2011. Journal of Clinical Virology 54: 342–348. - PubMed
-
- Gopalkrishna V, Patil PR, Patil GP, Chitambar SD (2012) Circulation of multiple enterovirus serotypes causing hand, foot and mouth disease in India. Journal of medical microbiology 61: 420–425. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
