

Adipose stem cells used to reconstruct 13 cases with cranio-maxillofacial hard-tissue defects
- PMID: 24558162
- PMCID: PMC3973720
- DOI: 10.5966/sctm.2013-0173
Adipose stem cells used to reconstruct 13 cases with cranio-maxillofacial hard-tissue defects
Abstract
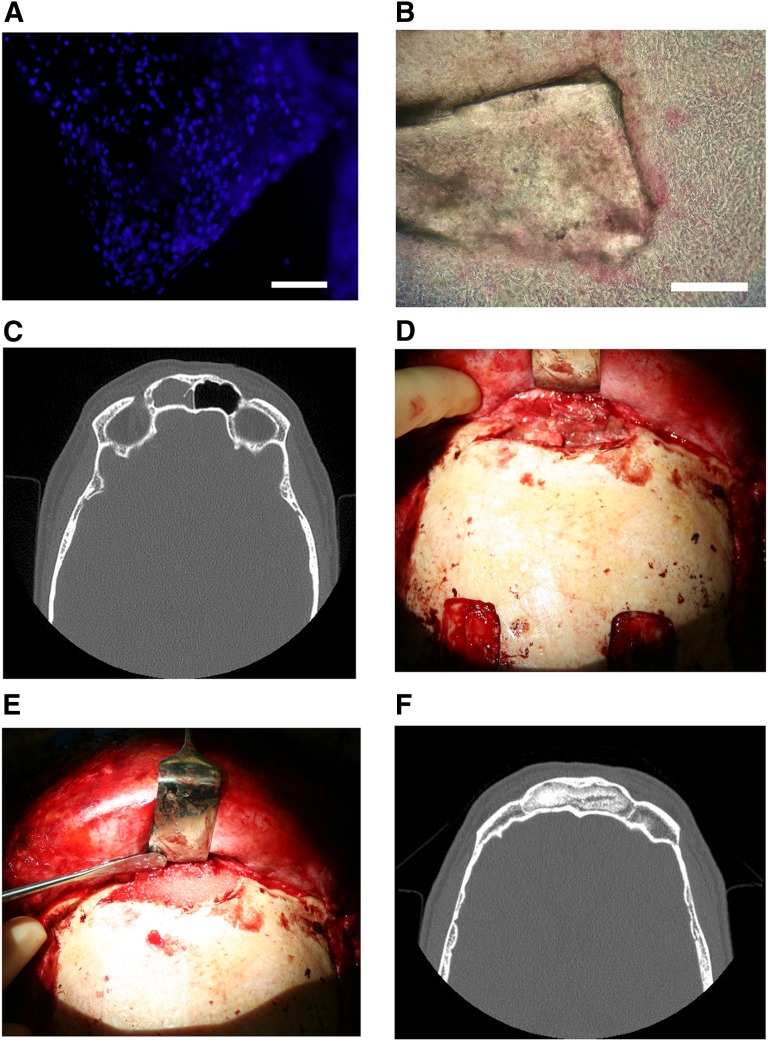
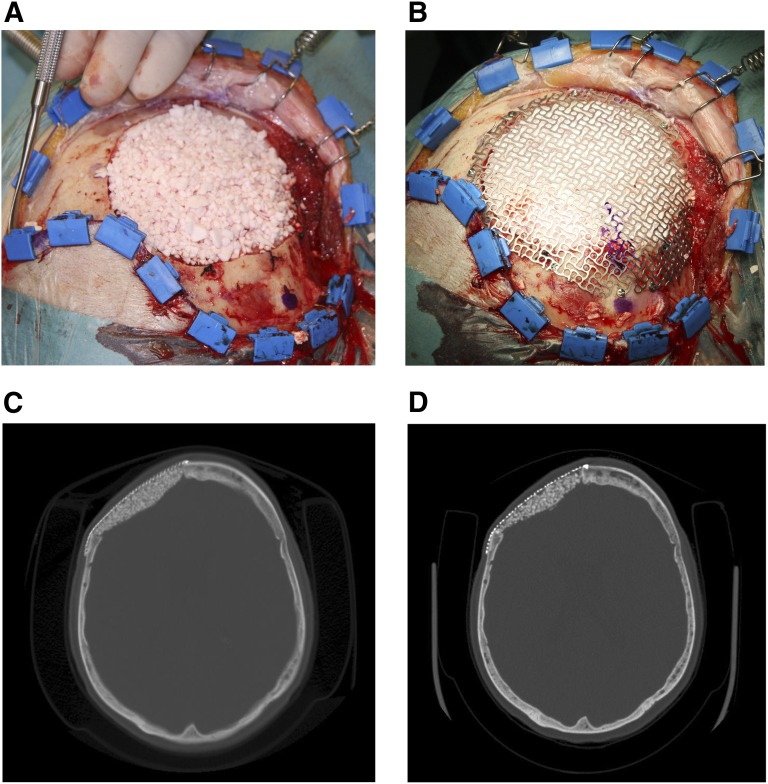
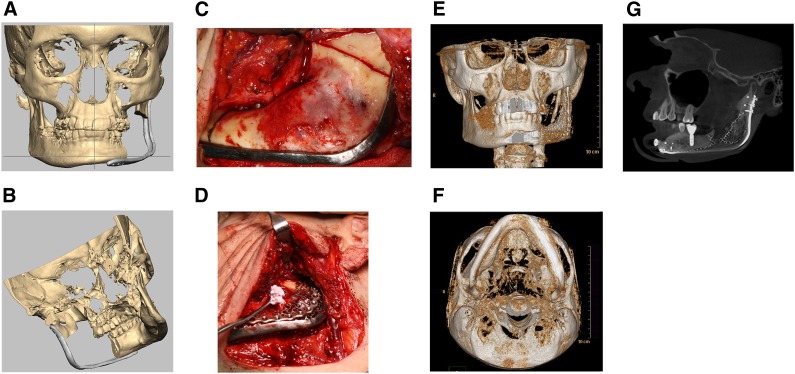
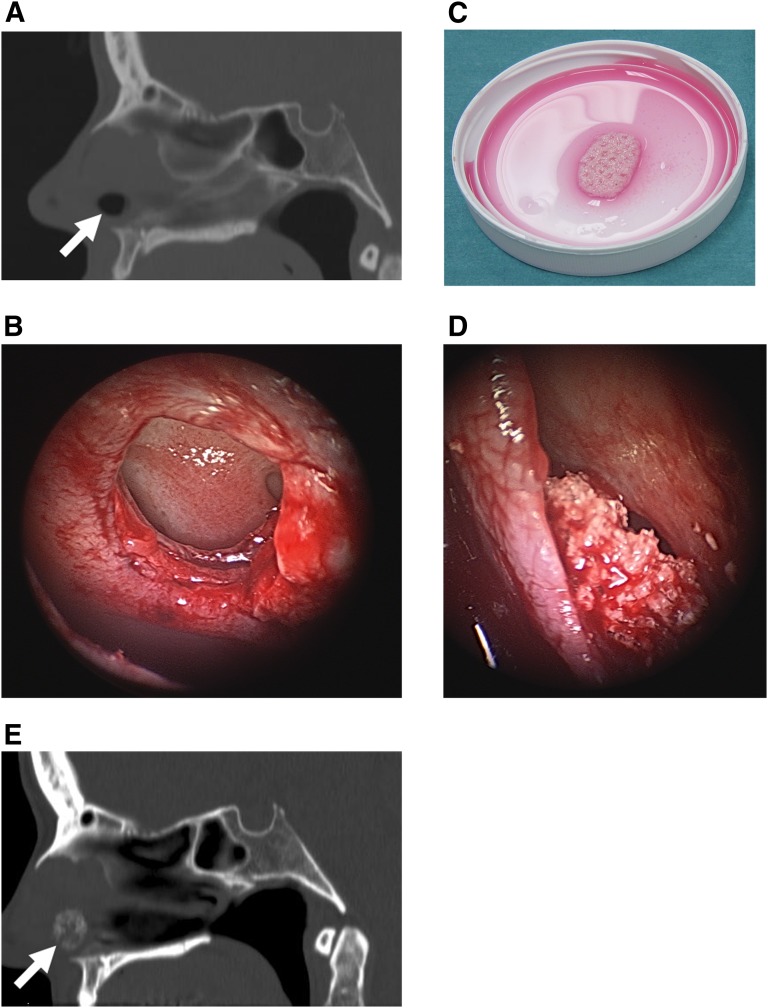
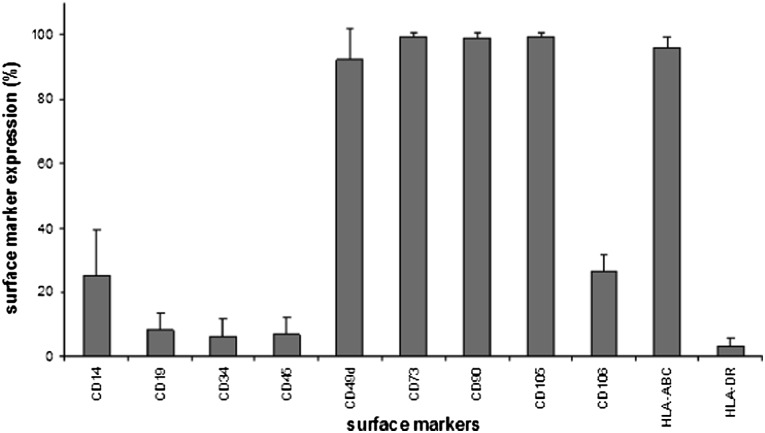
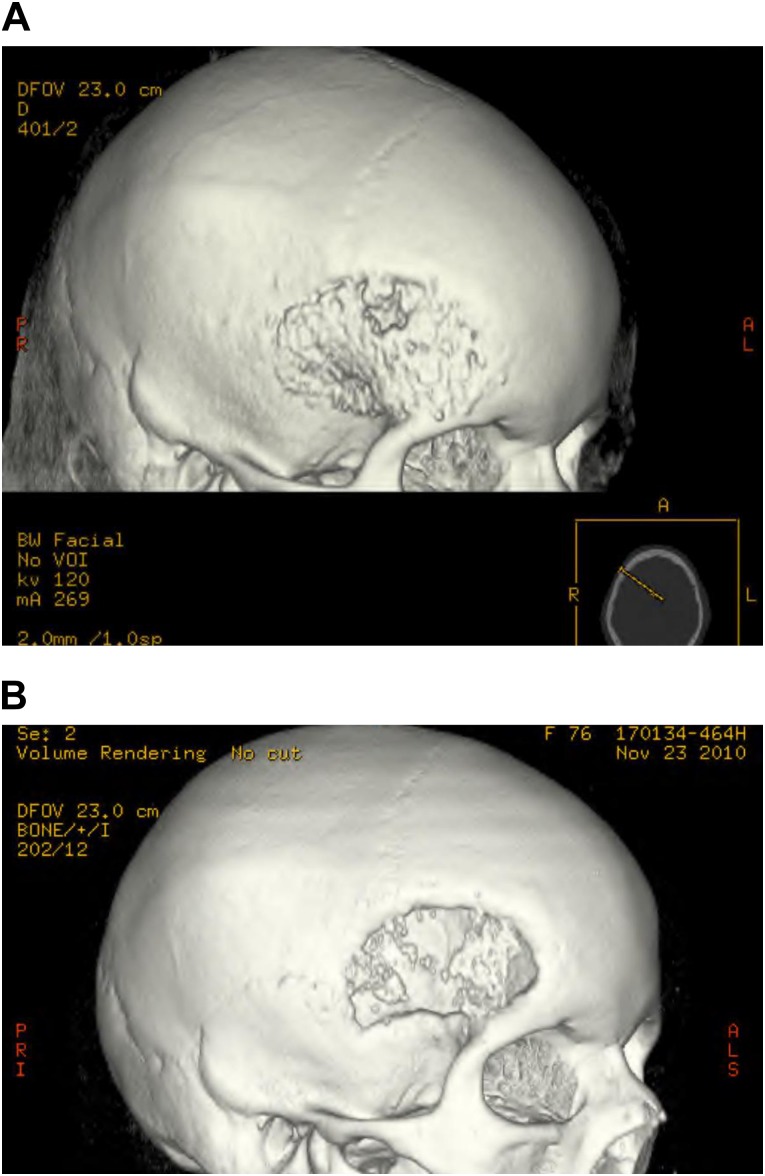
Although isolated reports of hard-tissue reconstruction in the cranio-maxillofacial skeleton exist, multipatient case series are lacking. This study aimed to review the experience with 13 consecutive cases of cranio-maxillofacial hard-tissue defects at four anatomically different sites, namely frontal sinus (3 cases), cranial bone (5 cases), mandible (3 cases), and nasal septum (2 cases). Autologous adipose tissue was harvested from the anterior abdominal wall, and adipose-derived stem cells were cultured, expanded, and then seeded onto resorbable scaffold materials for subsequent reimplantation into hard-tissue defects. The defects were reconstructed with either bioactive glass or β-tricalcium phosphate scaffolds seeded with adipose-derived stem cells (ASCs), and in some cases with the addition of recombinant human bone morphogenetic protein-2. Production and use of ASCs were done according to good manufacturing practice guidelines. Follow-up time ranged from 12 to 52 months. Successful integration of the construct to the surrounding skeleton was noted in 10 of the 13 cases. Two cranial defect cases in which nonrigid resorbable containment meshes were used sustained bone resorption to the point that they required the procedure to be redone. One septal perforation case failed outright at 1 year because of the postsurgical resumption of the patient's uncontrolled nasal picking habit.
Keywords: Adipose stem cells; Bioactive glass; Bone morphogenetic protein; β-Tricalcium phosphate.
Figures
Similar articles
-
Adipose stem cell tissue-engineered construct used to treat large anterior mandibular defect: a case report and review of the clinical application of good manufacturing practice-level adipose stem cells for bone regeneration.J Oral Maxillofac Surg. 2013 May;71(5):938-50. doi: 10.1016/j.joms.2012.11.014. Epub 2013 Feb 1. J Oral Maxillofac Surg. 2013. PMID: 23375899
-
Novel maxillary reconstruction with ectopic bone formation by GMP adipose stem cells.Int J Oral Maxillofac Surg. 2009 Mar;38(3):201-9. doi: 10.1016/j.ijom.2009.01.001. Epub 2009 Jan 24. Int J Oral Maxillofac Surg. 2009. PMID: 19168327
-
Cranioplasty with Adipose-Derived Stem Cells, Beta-Tricalcium Phosphate Granules and Supporting Mesh: Six-Year Clinical Follow-Up Results.Stem Cells Transl Med. 2017 Jul;6(7):1576-1582. doi: 10.1002/sctm.16-0410. Epub 2017 May 15. Stem Cells Transl Med. 2017. PMID: 28504874 Free PMC article.
-
Adipose stem cells and skeletal repair.Histol Histopathol. 2013 May;28(5):557-64. doi: 10.14670/HH-28.557. Epub 2012 Dec 21. Histol Histopathol. 2013. PMID: 23258367 Review.
-
Stem cells from adipose tissue.Cell Mol Biol Lett. 2011 Jun;16(2):236-57. doi: 10.2478/s11658-011-0005-0. Epub 2011 Mar 9. Cell Mol Biol Lett. 2011. PMID: 21394447 Free PMC article. Review.
Cited by
-
β-TCP from 3D-printed composite scaffolds acts as an effective phosphate source during osteogenic differentiation of human mesenchymal stromal cells.Front Cell Dev Biol. 2023 Oct 26;11:1258161. doi: 10.3389/fcell.2023.1258161. eCollection 2023. Front Cell Dev Biol. 2023. PMID: 37965582 Free PMC article.
-
Mesenchymal Stem Cell Therapy for Bone Regeneration.Clin Orthop Surg. 2018 Sep;10(3):271-278. doi: 10.4055/cios.2018.10.3.271. Epub 2018 Aug 22. Clin Orthop Surg. 2018. PMID: 30174801 Free PMC article. Review.
-
Scaffold Guided Bone Regeneration for the Treatment of Large Segmental Defects in Long Bones.Biomedicines. 2023 Jan 24;11(2):325. doi: 10.3390/biomedicines11020325. Biomedicines. 2023. PMID: 36830862 Free PMC article. Review.
-
Bioactive Herbal Extracts of Traditional Chinese Medicine Applied with the Biomaterials: For the Current Applications and Advances in the Musculoskeletal System.Front Pharmacol. 2021 Oct 28;12:778041. doi: 10.3389/fphar.2021.778041. eCollection 2021. Front Pharmacol. 2021. PMID: 34776987 Free PMC article. Review.
-
An Update on Adipose-Derived Stem Cells for Regenerative Medicine: Where Challenge Meets Opportunity.Adv Sci (Weinh). 2023 Jul;10(20):e2207334. doi: 10.1002/advs.202207334. Epub 2023 May 10. Adv Sci (Weinh). 2023. PMID: 37162248 Free PMC article. Review.
References
-
- Bianchi B, Ferri A, Ferrari S, et al. Mandibular resection and reconstruction in the management of extensive ameloblastoma. J Oral Maxillofac Surg. 2013;71:528–537. - PubMed
-
- Hidalgo DA. Fibula free flap: A new method of mandible reconstruction. Plast Reconstr Surg. 1989;84:71–79. - PubMed
-
- Sàndor GK, Nish IA, Carmichael RP. Comparison of conventional surgery with motorized trephine in bone harvest from the anterior iliac crest. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:150–155. - PubMed
-
- Ling XF, Peng X. What is the price to pay for a free fibula flap? A systematic review of donor-site morbidity following free fibula flap surgery. Plast Reconstr Surg. 2012;129:657–674. - PubMed
-
- Sieg P, Taner C, Hakim SG, et al. Long-term evaluation of donor site morbidity after free fibula transfer. Br J Oral Maxillofac Surg. 2010;48:267–270. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
