

Lowered testosterone in male obesity: mechanisms, morbidity and management
- PMID: 24407187
- PMCID: PMC3955331
- DOI: 10.4103/1008-682X.122365
Lowered testosterone in male obesity: mechanisms, morbidity and management
Abstract
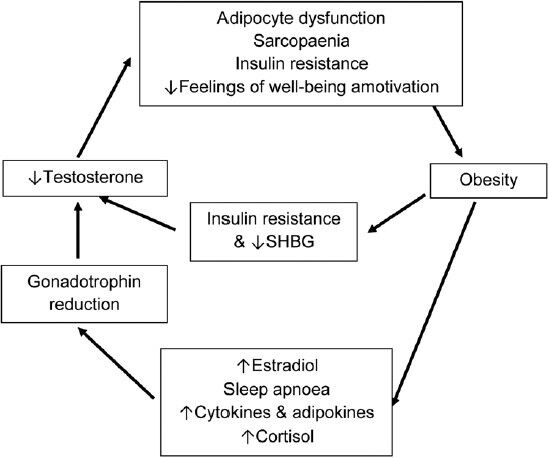
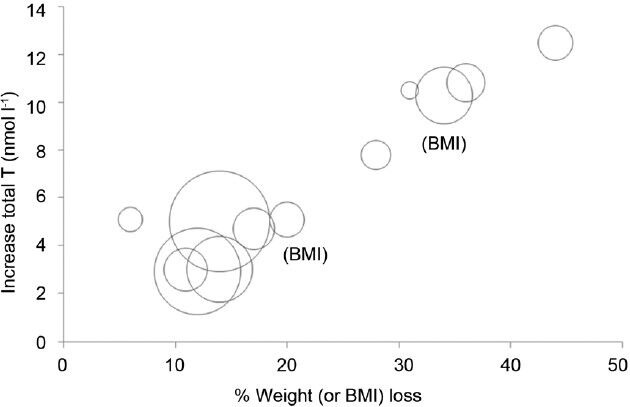
With increasing modernization and urbanization of Asia, much of the future focus of the obesity epidemic will be in the Asian region. Low testosterone levels are frequently encountered in obese men who do not otherwise have a recognizable hypothalamic-pituitary-testicular (HPT) axis pathology. Moderate obesity predominantly decreases total testosterone due to insulin resistance-associated reductions in sex hormone binding globulin. More severe obesity is additionally associated with reductions in free testosterone levels due to suppression of the HPT axis. Low testosterone by itself leads to increasing adiposity, creating a self-perpetuating cycle of metabolic complications. Obesity-associated hypotestosteronemia is a functional, non-permanent state, which can be reversible, but this requires substantial weight loss. While testosterone treatment can lead to moderate reductions in fat mass, obesity by itself, in the absence of symptomatic androgen defi ciency, is not an established indication for testosterone therapy. Testosterone therapy may lead to a worsening of untreated sleep apnea and compromise fertility. Whether testosterone therapy augments diet- and exercise-induced weight loss requires evaluation in adequately designed randomized controlled clinical trials.
Figures
Similar articles
-
Hypogonadism and male obesity: Focus on unresolved questions.Clin Endocrinol (Oxf). 2018 Jul;89(1):11-21. doi: 10.1111/cen.13723. Epub 2018 May 16. Clin Endocrinol (Oxf). 2018. PMID: 29683196 Review.
-
MANAGEMENT OF ENDOCRINE DISEASE: Rationale and current evidence for testosterone therapy in the management of obesity and its complications.Eur J Endocrinol. 2020 Dec;183(6):R167-R183. doi: 10.1530/EJE-20-0394. Eur J Endocrinol. 2020. PMID: 33105105 Review.
-
Late-onset hypogonadism: metabolic impact.Andrology. 2020 Nov;8(6):1519-1529. doi: 10.1111/andr.12705. Epub 2019 Sep 25. Andrology. 2020. PMID: 31502758 Review.
-
Testosterone and obesity.Obes Rev. 2015 Jul;16(7):581-606. doi: 10.1111/obr.12282. Epub 2015 May 15. Obes Rev. 2015. PMID: 25982085 Review.
-
Symptomatic response to testosterone treatment in dieting obese men with low testosterone levels in a randomized, placebo-controlled clinical trial.Int J Obes (Lond). 2017 Mar;41(3):420-426. doi: 10.1038/ijo.2016.242. Epub 2016 Dec 28. Int J Obes (Lond). 2017. PMID: 28028318 Clinical Trial.
Cited by
-
Bariatric Surgery: Remission of Inflammation, Cardiometabolic Benefits, and Common Adverse Effects.J Endocr Soc. 2020 Aug 4;4(9):bvaa049. doi: 10.1210/jendso/bvaa049. eCollection 2020 Sep 1. J Endocr Soc. 2020. PMID: 32775937 Free PMC article. Review.
-
The Impact of Diabetes on Male Silkworm Reproductive Health.Biology (Basel). 2024 Jul 24;13(8):557. doi: 10.3390/biology13080557. Biology (Basel). 2024. PMID: 39194495 Free PMC article.
-
Brain-derived neurotrophic factor, sex hormones and cognitive decline in male patients with schizophrenia receiving continuous antipsychotic therapy.World J Psychiatry. 2023 Dec 19;13(12):995-1004. doi: 10.5498/wjp.v13.i12.995. eCollection 2023 Dec 19. World J Psychiatry. 2023. PMID: 38186728 Free PMC article.
-
Hypogonadism and associated factors among male Leprosy patients.PLoS Negl Trop Dis. 2024 Aug 5;18(8):e0012374. doi: 10.1371/journal.pntd.0012374. eCollection 2024 Aug. PLoS Negl Trop Dis. 2024. PMID: 39102424 Free PMC article.
-
Long-term follow-up of gonadal dysfunction in morbidly obese adolescent boys after bariatric surgery.J Pediatr Endocrinol Metab. 2018 Nov 27;31(11):1191-1197. doi: 10.1515/jpem-2018-0261. J Pediatr Endocrinol Metab. 2018. PMID: 30352040 Free PMC article.
References
-
- WHO. WHO Global infobase, estimated overweight and obesity, 2002-2010 in males aged 30-100 y. [Last accessed on June 2013]. Available from: http://www.apps.who.int/infobase/Comparisons.aspx .
-
- Kelly T, Yang W, Chen CS, Reynolds K, He J. Global burden of obesity in 2005 and projections to 2030. Int J Obes (Lond) 2008;32:1431–7. - PubMed
-
- Tajar A, Forti G, O’Neill TW, Lee DM, Silman AJ, et al. Characteristics of secondary, primary, and compensated hypogonadism in aging men: evidence from the European Male Ageing Study. J Clin Endocrinol Metab. 2010;95:1810–8. - PubMed
-
- Heymsfield SB, Cefalu WT. Does body mass index adequately convey a patient's mortality risk? JAMA. 2013;309:87–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
