

Measurement of skeletal muscle radiation attenuation and basis of its biological variation
- PMID: 24393306
- PMCID: PMC4309522
- DOI: 10.1111/apha.12224
Measurement of skeletal muscle radiation attenuation and basis of its biological variation
Abstract
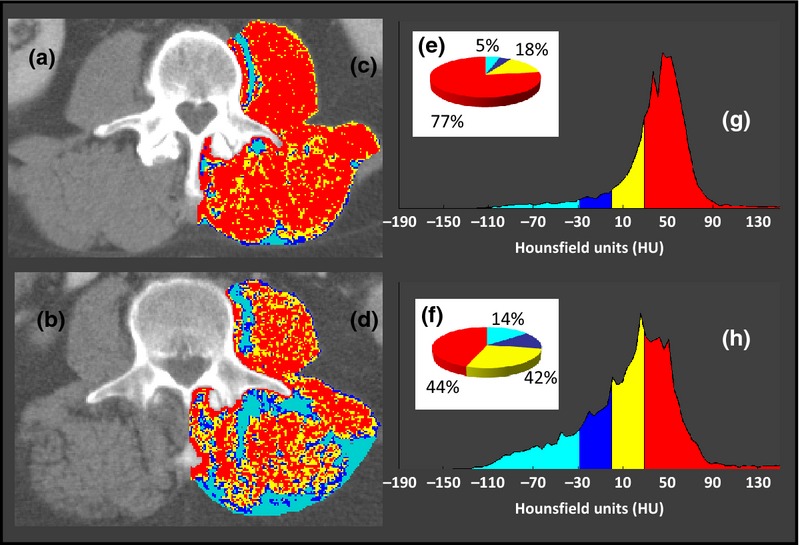
Skeletal muscle contains intramyocellular lipid droplets within the cytoplasm of myocytes as well as intermuscular adipocytes. These depots exhibit physiological and pathological variation which has been revealed with the advent of diagnostic imaging approaches: magnetic resonance (MR) imaging, MR spectroscopy and computed tomography (CT). CT uses computer-processed X-rays and is now being applied in muscle physiology research. The purpose of this review is to present CT methodologies and summarize factors that influence muscle radiation attenuation, a parameter which is inversely related to muscle fat content. Pre-defined radiation attenuation ranges are used to demarcate intermuscular adipose tissue [from -190 to -30 Hounsfield units (HU)] and muscle (-29 HU to +150 HU). Within the latter range, the mean muscle radiation attenuation [muscle (radio) density] is reported. Inconsistent criteria for the upper and lower HU cut-offs used to characterize muscle attenuation limit comparisons between investigations. This area of research would benefit from standardized criteria for reporting muscle attenuation. Available evidence suggests that muscle attenuation is plastic with physiological variation induced by the process of ageing, as well as by aerobic training, which probably reflects accumulation of lipids to fuel aerobic work. Pathological variation in muscle attenuation reflects excess fat deposition in the tissue and is observed in people with obesity, diabetes type II, myositis, osteoarthritis, spinal stenosis and cancer. A poor prognosis and different types of morbidity are predicted by the presence of reduced mean muscle attenuation values in patients with these conditions; however, the biological features of muscle with these characteristics require further investigation.
Keywords: Hounsfield units; computed tomography; muscle attenuation; muscle density; myosteatosis; skeletal muscle.
© 2014 The Authors. Acta Physiologica published by John Wiley & Sons Ltd on behalf of Scandinavian Physiological Society.
Figures
Similar articles
-
Low skeletal muscle radiation attenuation and visceral adiposity are associated with overall survival and surgical site infections in patients with pancreatic cancer.J Cachexia Sarcopenia Muscle. 2017 Apr;8(2):317-326. doi: 10.1002/jcsm.12155. Epub 2016 Oct 26. J Cachexia Sarcopenia Muscle. 2017. PMID: 27897432 Free PMC article.
-
Attenuation of skeletal muscle and strength in the elderly: The Health ABC Study.J Appl Physiol (1985). 2001 Jun;90(6):2157-65. doi: 10.1152/jappl.2001.90.6.2157. J Appl Physiol (1985). 2001. PMID: 11356778 Clinical Trial.
-
Composition of skeletal muscle evaluated with computed tomography.Ann N Y Acad Sci. 2000 May;904:18-24. doi: 10.1111/j.1749-6632.2000.tb06416.x. Ann N Y Acad Sci. 2000. PMID: 10865705 Review.
-
Skeletal muscle fat deposition is associated with hepatocellular carcinoma development in patients with chronic liver disease.Nutrition. 2018 Oct;54:83-88. doi: 10.1016/j.nut.2018.03.011. Epub 2018 Mar 21. Nutrition. 2018. PMID: 29753174
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
Cited by
-
Sarcopenia in the Older Adult With Cancer.J Clin Oncol. 2021 Jul 1;39(19):2068-2078. doi: 10.1200/JCO.21.00102. Epub 2021 May 27. J Clin Oncol. 2021. PMID: 34043430 Free PMC article. Review. No abstract available.
-
Myosteatosis: Diagnosis, pathophysiology and consequences in metabolic dysfunction-associated steatotic liver disease.JHEP Rep. 2023 Nov 14;6(2):100963. doi: 10.1016/j.jhepr.2023.100963. eCollection 2024 Feb. JHEP Rep. 2023. PMID: 38322420 Free PMC article. Review.
-
A computed tomography study investigating the effects of botulinum toxin injections prior to complex abdominal wall reconstruction.Hernia. 2023 Apr;27(2):281-291. doi: 10.1007/s10029-022-02692-w. Epub 2022 Oct 14. Hernia. 2023. PMID: 36239824 Free PMC article.
-
Age-related fatty infiltration of lumbar paraspinal muscles: a normative reference database study in 516 Chinese females.Quant Imaging Med Surg. 2020 Aug;10(8):1590-1601. doi: 10.21037/qims-19-835. Quant Imaging Med Surg. 2020. PMID: 32742954 Free PMC article.
-
Three-dimensional body composition parameters using automatic volumetric segmentation allow accurate prediction of colorectal cancer outcomes.J Cachexia Sarcopenia Muscle. 2024 Feb;15(1):281-291. doi: 10.1002/jcsm.13404. Epub 2023 Dec 20. J Cachexia Sarcopenia Muscle. 2024. PMID: 38123148 Free PMC article.
References
-
- Airaksinen O, Herno A, Kaukanen E, Saari T, Sihvonen T, Suomalainen O. Density of lumbar muscles 4 years after decompressive spinal surgery. Eur Spine J. 1996;5:193–197. - PubMed
-
- Antoun S, Lanoy E, Lacovelli R, Albides-Sauvin L, Loriot Y, Merad-Taoufik M, Fizazi K, di Palma M, Baracos VE, Escudier B. Skeletal muscle density predicts prognosis in patients with metastatic renal cell carcinoma treated with targeted therapies. Cancer. 2013;119:3377–3384. - PubMed
-
- Baumgartner RN. Body composition in healthy aging. Ann N Y Acad Sci. 2000;904:437–448. - PubMed
-
- Berg HE, Tedner B, Tesch PA. Changes in lower limb muscle cross-sectional area and tissue fluid volume after transition from standing to supine. Acta Physiol Scand. 1993;148:379–385. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
