

Immunologic predictors of coronary artery calcium progression in a contemporary HIV cohort
- PMID: 24370480
- PMCID: PMC4199584
- DOI: 10.1097/QAD.0000000000000145
Immunologic predictors of coronary artery calcium progression in a contemporary HIV cohort
Abstract
Background: Identifying immunologic mechanisms that contribute to premature cardiovascular disease (CVD) among HIV-positive patients will inform prevention strategies.
Methods: Coronary artery calcium (CAC) progression was studied in an HIV cohort. Immunophenotypes were measured on baseline cryopreserved peripheral blood mononuclear cells using multicolor flow cytometry. Logistic regression identified predictors of CAC progression after adjusting for traditional and HIV-related risk factors.
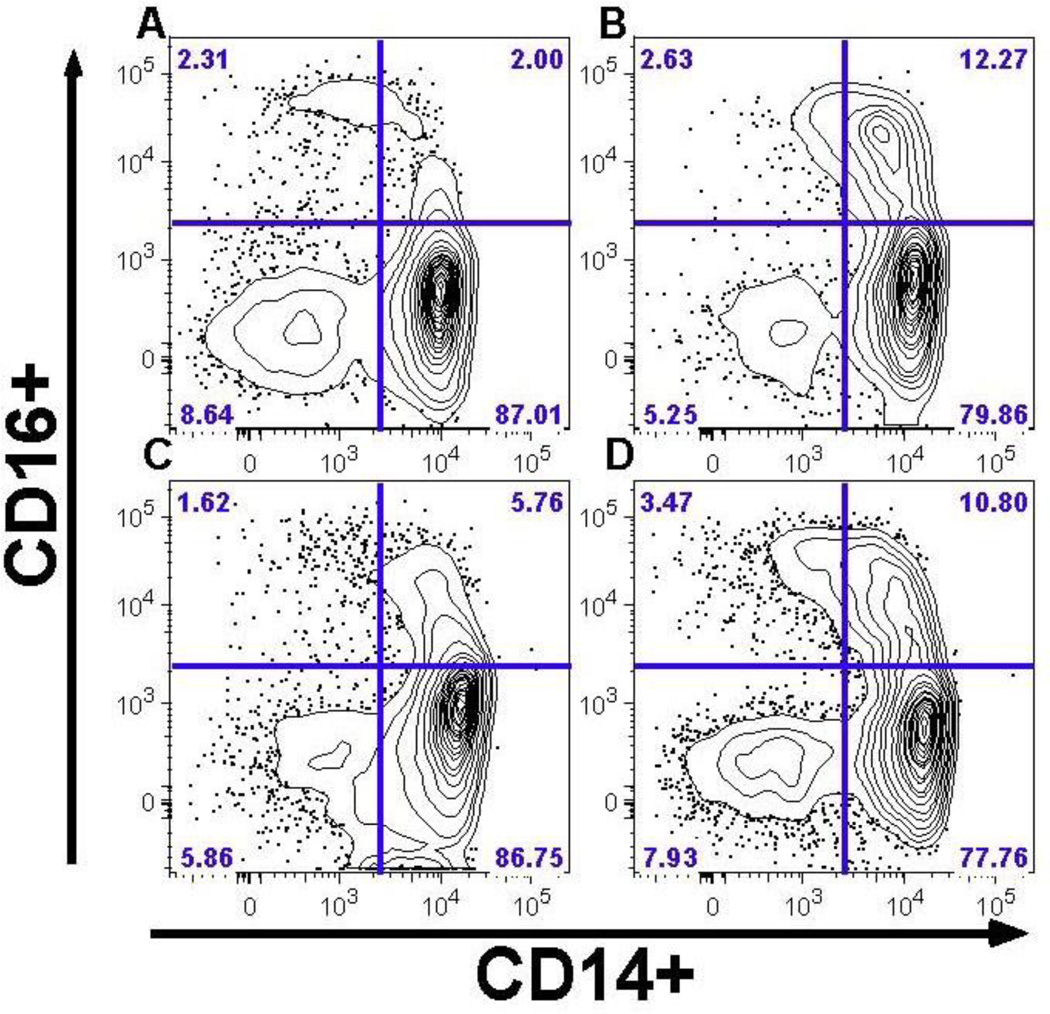
Results: Baseline characteristics for the analysis cohort (n=436) were median age 42 years, median CD4 cell count 481 cells/μl, and 78% receiving antiretroviral therapy. Higher frequencies of CD16 monocytes were associated with greater likelihood of CAC progression, after adjusting for traditional and HIV risk factors [odds ratio per doubling was 1.66 for CD14/CD16 (P=0.02), 1.36 for CD14/CD16 (P=0.06), and 1.69 for CD14/CD16 (P=0.01)]. Associations for CD16 monocytes persisted when restricted to participants with viral suppression. We found no significant associations for CAC progression with other cellular phenotypes, including T-cell activation and senescence markers.
Conclusion: Circulating CD16 monocytes, potentially reflecting a more pro-atherogenic subpopulation, independently predicted greater CAC progression among HIV-infected persons at low risk for AIDS. In contrast to T-cell abnormalities classically associated with AIDS-related disease progression, these data highlight the potential role of monocyte activation in HIV-related CVD risk.
Conflict of interest statement
Figures
Similar articles
-
Non-classical monocytes predict progression of carotid artery bifurcation intima-media thickness in HIV-infected individuals on stable antiretroviral therapy.HIV Clin Trials. 2016 May;17(3):114-22. doi: 10.1080/15284336.2016.1162386. Epub 2016 Apr 4. HIV Clin Trials. 2016. PMID: 27125366 Free PMC article.
-
Non-Classical Monocytes and Monocyte Chemoattractant Protein-1 (MCP-1) Correlate with Coronary Artery Calcium Progression in Chronically HIV-1 Infected Adults on Stable Antiretroviral Therapy.PLoS One. 2016 Feb 11;11(2):e0149143. doi: 10.1371/journal.pone.0149143. eCollection 2016. PLoS One. 2016. PMID: 26867220 Free PMC article.
-
Association of Elevations of Specific T Cell and Monocyte Subpopulations in Rheumatoid Arthritis With Subclinical Coronary Artery Atherosclerosis.Arthritis Rheumatol. 2016 Jan;68(1):92-102. doi: 10.1002/art.39419. Arthritis Rheumatol. 2016. PMID: 26360530 Free PMC article.
-
Incidence and progression of coronary artery calcium in HIV-infected and HIV-uninfected men.AIDS. 2015 Nov 28;29(18):2427-34. doi: 10.1097/QAD.0000000000000847. AIDS. 2015. PMID: 26558542 Free PMC article.
-
Plasma monocyte chemoattractant protein-1 and tumor necrosis factor-α levels predict the presence of coronary artery calcium in HIV-infected individuals independent of traditional cardiovascular risk factors.AIDS Res Hum Retroviruses. 2014 Feb;30(2):142-6. doi: 10.1089/AID.2013.0183. Epub 2013 Sep 21. AIDS Res Hum Retroviruses. 2014. PMID: 23984974 Free PMC article.
Cited by
-
The CD14 C-260T single nucleotide polymorphism (SNP) modulates monocyte/macrophage activation in treated HIV-infected individuals.J Transl Med. 2015 Jan 27;13:30. doi: 10.1186/s12967-015-0391-6. J Transl Med. 2015. PMID: 25622527 Free PMC article.
-
Early Antiretroviral Therapy at High CD4 Counts Does Not Improve Arterial Elasticity: A Substudy of the Strategic Timing of AntiRetroviral Treatment (START) Trial.Open Forum Infect Dis. 2016 Oct 8;3(4):ofw213. doi: 10.1093/ofid/ofw213. eCollection 2016 Oct. Open Forum Infect Dis. 2016. PMID: 27942541 Free PMC article.
-
Loss of CXCR4 on non-classical monocytes in participants of the Women's Interagency HIV Study (WIHS) with subclinical atherosclerosis.Cardiovasc Res. 2019 May 1;115(6):1029-1040. doi: 10.1093/cvr/cvy292. Cardiovasc Res. 2019. PMID: 30520941 Free PMC article.
-
PD-1+ and TIGIT+ CD4 T Cells Are Associated With Coronary Artery Calcium Progression in HIV-Infected Treated Adults.J Acquir Immune Defic Syndr. 2019 May 1;81(1):e21-e23. doi: 10.1097/QAI.0000000000002001. J Acquir Immune Defic Syndr. 2019. PMID: 30865177 Free PMC article. No abstract available.
-
Ageing with HIV.Healthcare (Basel). 2018 Feb 14;6(1):17. doi: 10.3390/healthcare6010017. Healthcare (Basel). 2018. PMID: 29443936 Free PMC article. Review.
References
-
- Mocroft A, Reiss P, Gasiorowski J, Ledergerber B, Kowalska J, Chiesi A, et al. Serious fatal and nonfatal non-AIDS-defining illnesses in Europe. J Acquir Immune Defic Syndr. 2010;55:262–270. - PubMed
-
- El-Sadr WM, Lundgren JD, Neaton JD, Gordin F, Abrams D, Arduino RC, et al. CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med. 2006;355:2283–2296. - PubMed
-
- Friis-Moller N, Reiss P, Sabin CA, Weber R, Monforte A, El-Sadr W, et al. Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med. 2007;356:1723–1735. - PubMed
-
- Saves M, Chene G, Ducimetiere P, Leport C, Le Moal G, Amouyel P, et al. Risk Factors for coronary heart disease in patients treated for human immunodeficiency virus infection compared with the general population. CID. 2003;37:292–298. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
