

Epitope analysis of the collagen type V-specific T cell response in lung transplantation reveals an HLA-DRB1*15 bias in both recipient and donor
- PMID: 24265781
- PMCID: PMC3827168
- DOI: 10.1371/journal.pone.0079601
Epitope analysis of the collagen type V-specific T cell response in lung transplantation reveals an HLA-DRB1*15 bias in both recipient and donor
Abstract
Background: IL-17-dependent cellular immune responses to the α1 chain of collagen type V are associated with development of bronchiolitis obliterans syndrome after lung transplantation, and with idiopathic pulmonary fibrosis and coronary artery disease, primary indications for lung or heart transplantation, respectively.
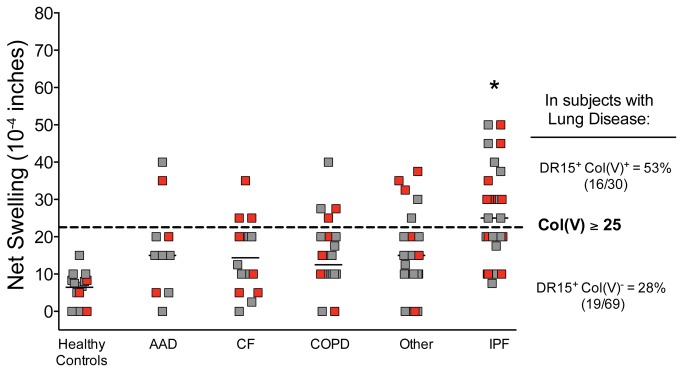
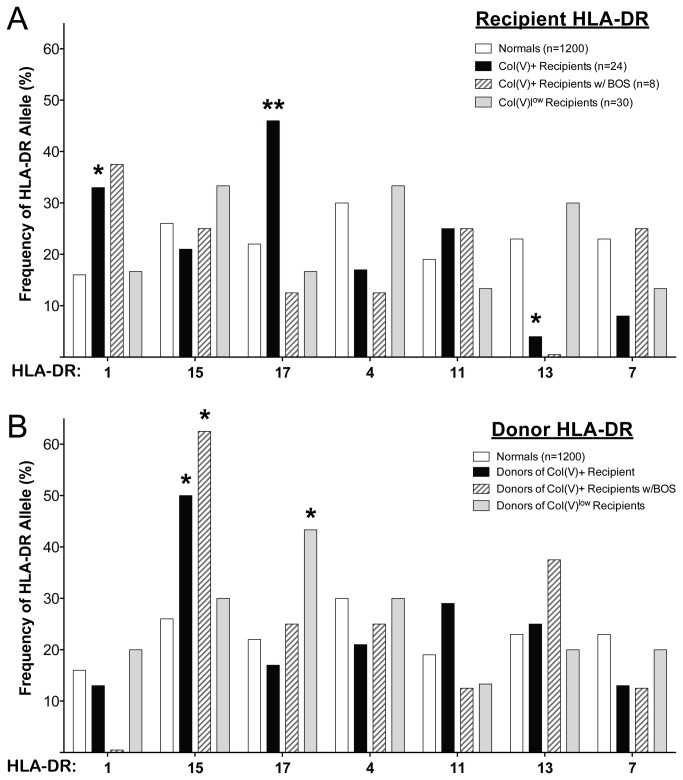
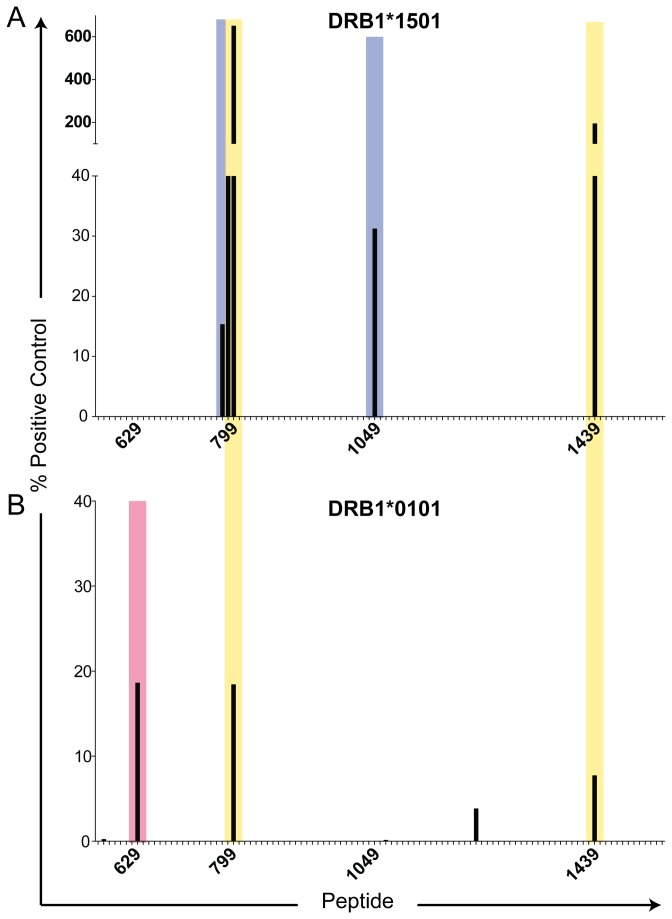
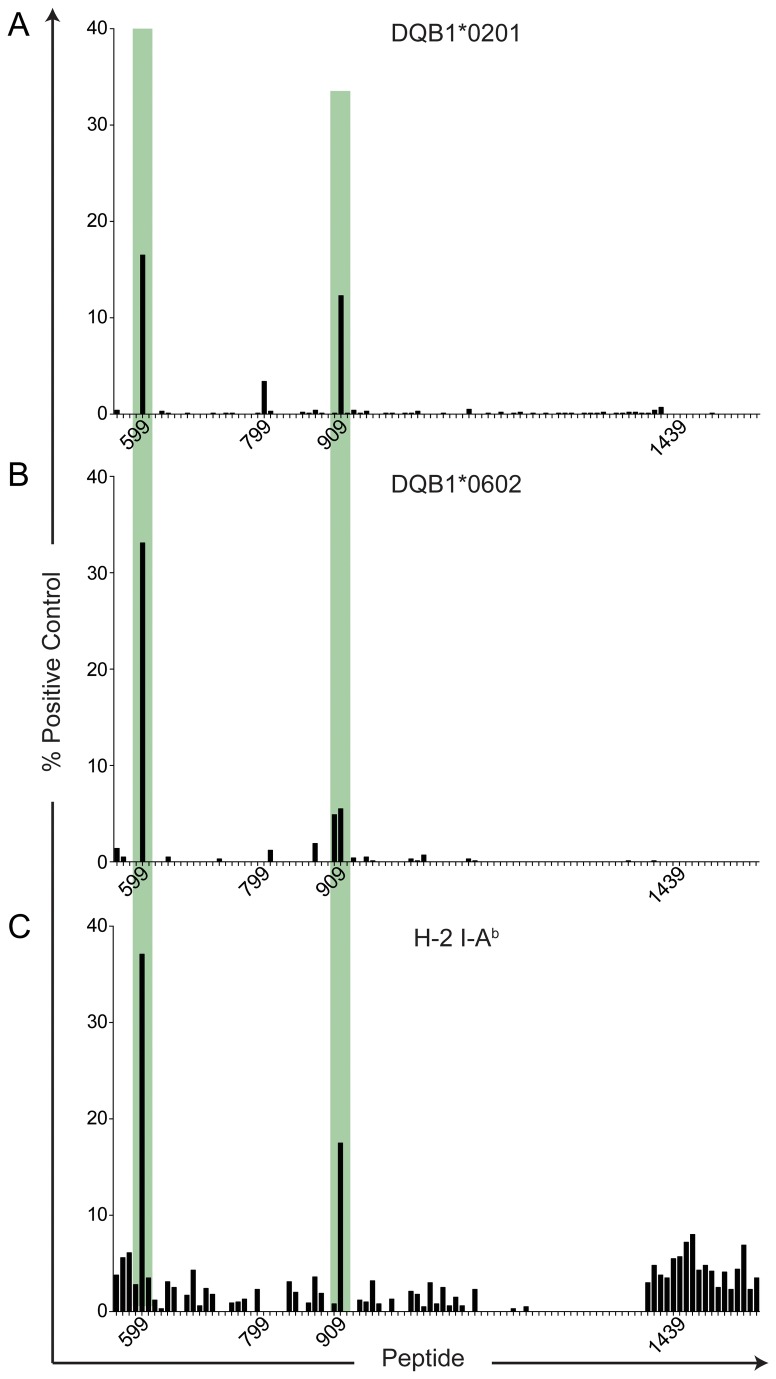
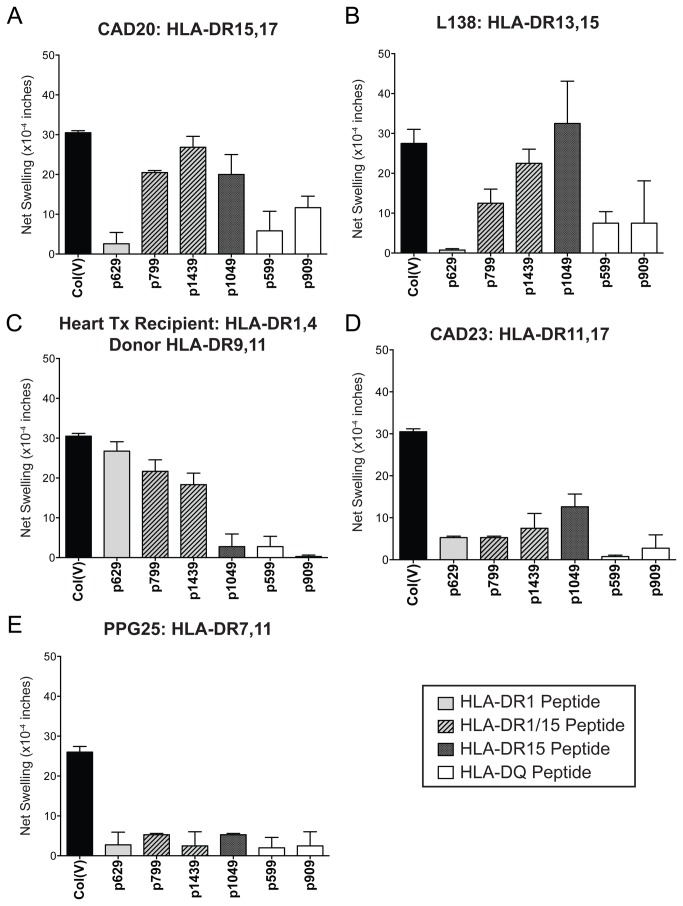
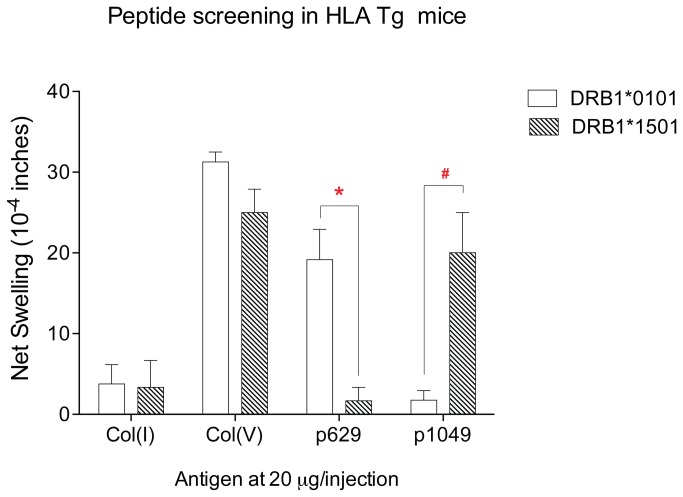
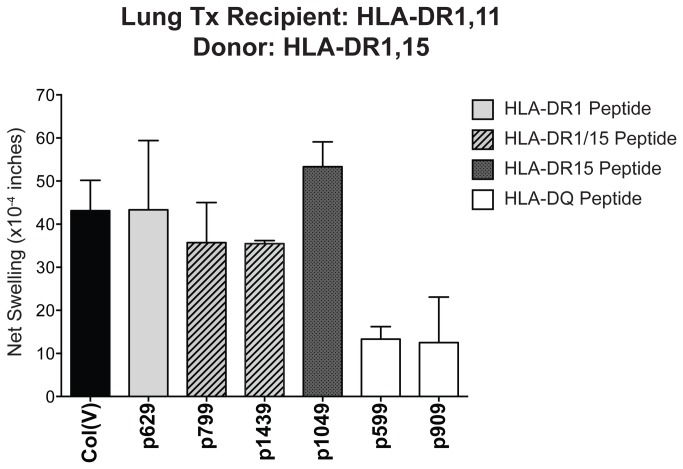
Methodology/principal findings: We found that 30% of the patients awaiting lung transplantation exhibited a strong cell-mediated immune response to col(V). Of these, 53% expressed HLA-DR15, compared to a 28% HLA-DR15 frequency in col(V) low-responders (p=0.02). After transplantation, patients with HLA-DR1 and -DR17, not -DR15, developed anti-col(V) responses most frequently (p=0.04 and 0.01 vs. controls, respectively). However, recipients of a lung from an HLA-DR15(+)donor were at significantly elevated risk of developing anti-col(V) responses (p=0.02) and BOS (p=0.03). To determine the molecular basis of this unusual pattern of DR allele bias, a peptide library comprising the collagenous region of the α1(V) protein was screened for binding to HLA-DR0101, -DR1501, -DR0301 (DR17) or to HLA-DQ2 (DQA1*0501: DQB1*0201; in linkage disequilibrium with -DR17) and -DQ6 (DQA1*0102: DQB1*0602; linked to -DR15). Eight 15-mer peptides, six DR-binding and two DQ-binding, were identified. HLA-DR15 binding to two peptides yielded the highest binding scores: 650 (where 100 = positive control) for p799 (GIRGLKGTKGEKGED), and 193 for p1439 (LRGIPGPVGEQGLPG). These peptides, which also bound weakly to HLA-DR1, elicited responses in both HLA-DR1(+) and -DR15(+) col(V) reactive hosts, whereas binding and immunoreactivity of p1049 (KDGPPGLRGFPGDRG) was DR15-specific. Remarkably, a col(V)-reactive HLA-DR1(+)DR15(neg) lung transplant patient, whose donor was HLA-DR15(+), responded not only to p799 and p1439, but also to p1049.
Conclusions/significance: HLA-DR15 and IPF disease were independently associated with pre-transplant col(V) autoimmunity. The increased risk of de novo immunity to col(V) and BOS, associated with receiving a lung transplant from an HLA-DR15(+) donor, may result from presentation by donor-derived HLA- DR15, of novel self-peptides to recipient T cells.
Conflict of interest statement
Figures
Similar articles
-
Donor HLA-DR Drives the Development of De Novo Autoimmunity Following Lung and Heart Transplantation.Transplant Direct. 2020 Sep 24;6(10):e607. doi: 10.1097/TXD.0000000000001062. eCollection 2020 Oct. Transplant Direct. 2020. PMID: 33062840 Free PMC article.
-
Specific Donor HLA-DR Types Correlate With Altered Susceptibility to Development of Chronic Lung Allograft Dysfunction.Transplantation. 2018 Jul;102(7):1132-1138. doi: 10.1097/TP.0000000000002107. Transplantation. 2018. PMID: 29360666 Free PMC article.
-
A shift in the collagen V antigenic epitope leads to T helper phenotype switch and immune response to self-antigen leading to chronic lung allograft rejection.Clin Exp Immunol. 2012 Jan;167(1):158-68. doi: 10.1111/j.1365-2249.2011.04486.x. Clin Exp Immunol. 2012. PMID: 22132895 Free PMC article.
-
Role of autoimmunity in organ allograft rejection: a focus on immunity to type V collagen in the pathogenesis of lung transplant rejection.Am J Physiol Lung Cell Mol Physiol. 2004 Jun;286(6):L1129-39. doi: 10.1152/ajplung.00330.2003. Am J Physiol Lung Cell Mol Physiol. 2004. PMID: 15136293 Review.
-
Regulatory T cells in lung transplantation--an emerging concept.Semin Immunopathol. 2011 Mar;33(2):117-27. doi: 10.1007/s00281-011-0253-0. Epub 2011 Mar 20. Semin Immunopathol. 2011. PMID: 21424593 Free PMC article. Review.
Cited by
-
Donor HLA-DR Drives the Development of De Novo Autoimmunity Following Lung and Heart Transplantation.Transplant Direct. 2020 Sep 24;6(10):e607. doi: 10.1097/TXD.0000000000001062. eCollection 2020 Oct. Transplant Direct. 2020. PMID: 33062840 Free PMC article.
-
Differential requirement for P2X7R function in IL-17 dependent vs. IL-17 independent cellular immune responses.Am J Transplant. 2014 Jul;14(7):1512-22. doi: 10.1111/ajt.12741. Epub 2014 May 27. Am J Transplant. 2014. PMID: 24866539 Free PMC article.
-
Idiopathic pulmonary fibrosis beyond the lung: understanding disease mechanisms to improve diagnosis and management.Respir Res. 2021 Apr 17;22(1):109. doi: 10.1186/s12931-021-01711-1. Respir Res. 2021. PMID: 33865386 Free PMC article. Review.
-
Basement membranes and autoimmune diseases.Matrix Biol. 2017 Jan;57-58:149-168. doi: 10.1016/j.matbio.2016.07.008. Epub 2016 Aug 2. Matrix Biol. 2017. PMID: 27496347 Free PMC article. Review.
-
Mucosal Administration of Collagen V Ameliorates the Atherosclerotic Plaque Burden by Inducing Interleukin 35-dependent Tolerance.J Biol Chem. 2016 Feb 12;291(7):3359-70. doi: 10.1074/jbc.M115.681882. Epub 2015 Dec 31. J Biol Chem. 2016. PMID: 26721885 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
