

The activity of circulating dipeptidyl peptidase-4 is associated with subclinical left ventricular dysfunction in patients with type 2 diabetes mellitus
- PMID: 24099410
- PMCID: PMC3852480
- DOI: 10.1186/1475-2840-12-143
The activity of circulating dipeptidyl peptidase-4 is associated with subclinical left ventricular dysfunction in patients with type 2 diabetes mellitus
Abstract
Background: Patients with type 2 diabetes mellitus (T2DM) present subclinical left ventricular systolic and/or diastolic dysfunction (LVD). Dipeptidyl peptidase-4 (DPP4) inactivates peptides that possess cardioprotective actions. Our aim was to analyze whether the activity of circulating DPP4 is associated with echocardiographically defined LVD in asymptomatic patients with T2DM.
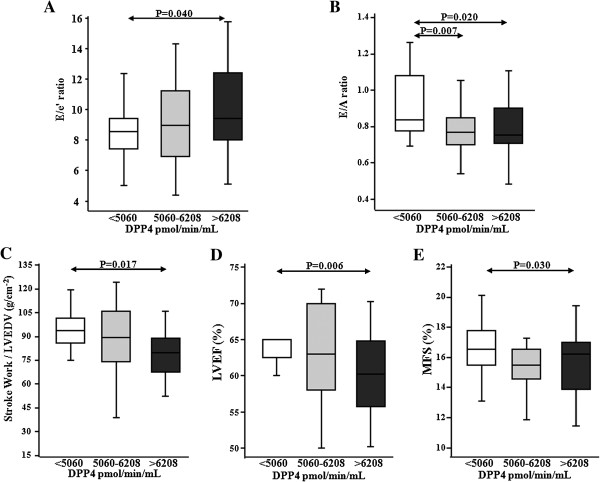
Methods: In this cross-sectional study, we examined 83 T2DM patients with no coronary or valve heart disease and 59 age and gender-matched non-diabetic subjects. Plasma DPP4 activity (DPP4a) was measured by enzymatic assay and serum amino-terminal pro-brain natriuretic peptide (NT-proBNP) was measured by enzyme-linked immunosorbent assay. LV function was assessed by two-dimensional echocardiographic imaging, targeted M-mode recordings and Doppler ultrasound measurements. Differences in means were assessed by t-tests and one-way ANOVA. Associations were assessed by adjusted multiple linear regression and logistic regression analyses.
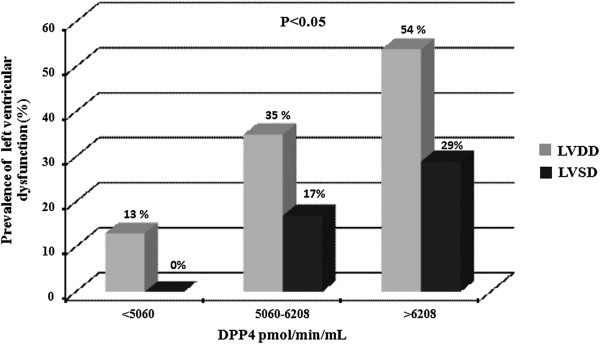
Results: DPP4a was increased in T2DM patients as compared with non-diabetic subjects (5855 ± 1632 vs 5208 ± 957 pmol/min/mL, p < 0.05). Clinical characteristics and echocardiographic parameters assessing LV morphology were similar across DPP4a tertiles in T2DM patients. However, prevalence of LVD progressively increased across incremental DPP4a tertiles (13%, 39% and 71%, all p < 0.001). Multivariate regression analysis confirmed the independent associations of DPP4a with LVD in T2DM patients (p < 0.05). Similarly, multiple logistic regression analysis showed that an increase of 100 pmol/min/min plasma DPP4a was independently associated with an increased frequency of LVD with an adjusted odds ratio of 1.10 (95% CI, 1.04 to 1.15, p = 0.001).
Conclusions: An excessive activity of circulating DPP4 is independently associated with subclinical LVD in T2DM patients. Albeit descriptive, these findings suggest that DPP4 may be involved in the mechanisms of LVD in T2DM.
Figures
Comment on
-
The neurogenic response of cardiac resident nestin(+) cells was associated with GAP43 upregulation and abrogated in a setting of type I diabetes.Cardiovasc Diabetol. 2013 Aug 12;12:114. doi: 10.1186/1475-2840-12-114. Cardiovasc Diabetol. 2013. PMID: 23938193 Free PMC article.
Similar articles
-
The neurogenic response of cardiac resident nestin(+) cells was associated with GAP43 upregulation and abrogated in a setting of type I diabetes.Cardiovasc Diabetol. 2013 Aug 12;12:114. doi: 10.1186/1475-2840-12-114. Cardiovasc Diabetol. 2013. PMID: 23938193 Free PMC article.
-
Plasma dipeptidyl-peptidase-4 activity is associated with left ventricular systolic function in patients with ST-segment elevation myocardial infarction.Sci Rep. 2017 Jul 21;7(1):6097. doi: 10.1038/s41598-017-06514-3. Sci Rep. 2017. PMID: 28733630 Free PMC article.
-
Prognostic value of plasma DPP4 activity in ST-elevation myocardial infarction.Cardiovasc Diabetol. 2017 Jun 6;16(1):72. doi: 10.1186/s12933-017-0553-3. Cardiovasc Diabetol. 2017. PMID: 28587613 Free PMC article.
-
NT-proBNP, echocardiographic abnormalities and subclinical coronary artery disease in high risk type 2 diabetic patients.Cardiovasc Diabetol. 2012 Mar 5;11:19. doi: 10.1186/1475-2840-11-19. Cardiovasc Diabetol. 2012. PMID: 22390472 Free PMC article.
-
DPP4 Inhibition Ameliorates Cardiac Function by Blocking the Cleavage of HMGB1 in Diabetic Mice After Myocardial Infarction.Int Heart J. 2017 Oct 21;58(5):778-786. doi: 10.1536/ihj.16-547. Epub 2017 Sep 30. Int Heart J. 2017. PMID: 28966327
Cited by
-
Dipeptidyl peptidase inhibition prevents diastolic dysfunction and reduces myocardial fibrosis in a mouse model of Western diet induced obesity.Metabolism. 2014 Aug;63(8):1000-11. doi: 10.1016/j.metabol.2014.04.002. Epub 2014 Apr 12. Metabolism. 2014. PMID: 24933400 Free PMC article.
-
Clinical features of subclinical left ventricular systolic dysfunction in patients with diabetes mellitus.Cardiovasc Diabetol. 2015 Apr 17;14:37. doi: 10.1186/s12933-015-0201-8. Cardiovasc Diabetol. 2015. PMID: 25889250 Free PMC article.
-
Reduced post-operative DPP4 activity associated with worse patient outcome after cardiac surgery.Sci Rep. 2018 Aug 7;8(1):11820. doi: 10.1038/s41598-018-30235-w. Sci Rep. 2018. PMID: 30087386 Free PMC article.
-
Pleiotropic effects of the dipeptidylpeptidase-4 inhibitors on the cardiovascular system.Am J Physiol Heart Circ Physiol. 2014 Aug 15;307(4):H477-92. doi: 10.1152/ajpheart.00209.2014. Am J Physiol Heart Circ Physiol. 2014. PMID: 24929856 Free PMC article. Review.
-
Targeting metabolic disturbance in the diabetic heart.Cardiovasc Diabetol. 2015 Feb 7;14:17. doi: 10.1186/s12933-015-0173-8. Cardiovasc Diabetol. 2015. PMID: 25856422 Free PMC article. Review.
References
-
- Chareonthaitawee P, Sorajja P, Rajagopalan N, Miller TD, Hodge DO, Frye RL, Gibbons RJ. Prevalence and prognosis of left ventricular systolic dysfunction in asymptomatic diabetic patients without known coronary artery disease referred for stress single-photon emission computed tomography and assessment of left ventricular function. Am Heart J. 2007;154:567–574. doi: 10.1016/j.ahj.2007.04.042. - DOI - PubMed
-
- Giorda CB, Cioffi G, de Simone G, Di Lenarda A, Faggiano P, Latini R, Lucci D, Maggioni AP, Tarantini L, Velussi M, Verdecchia P, Comaschi M. on behalf of the DYDA study. Predictors of early-stage left ventricular dysfunction in type 2 diabetes: results of DYDA study. Eur J Cardiovasc Prev Rehabil. 2011;18:415–423. doi: 10.1177/1741826710389402. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
