

Treatment challenges in the management of relapsed or refractory non-Hodgkin's lymphoma - novel and emerging therapies
- PMID: 24049458
- PMCID: PMC3775637
- DOI: 10.2147/CMAR.S34273
Treatment challenges in the management of relapsed or refractory non-Hodgkin's lymphoma - novel and emerging therapies
Abstract
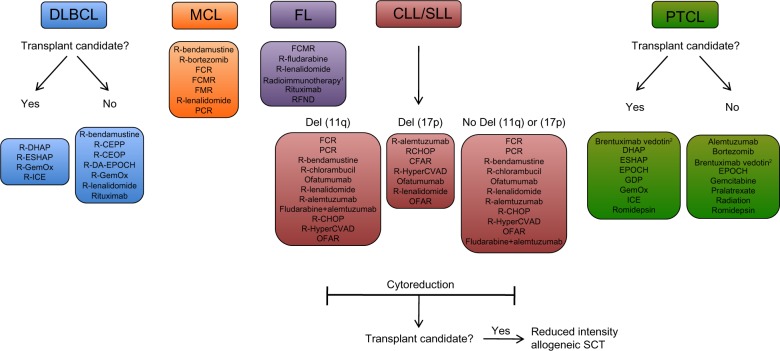
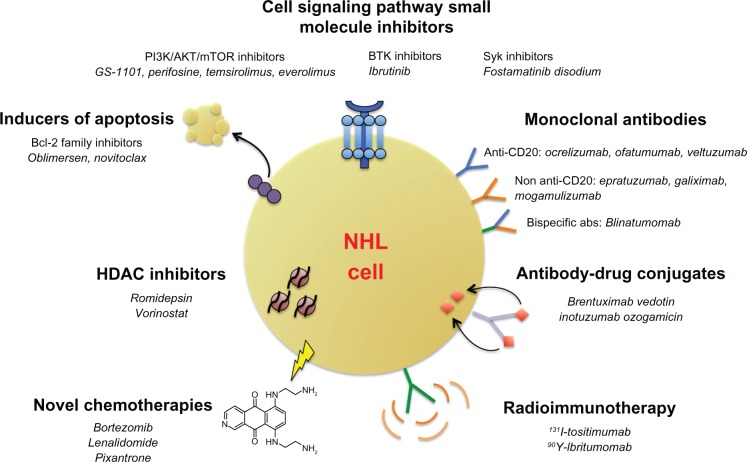
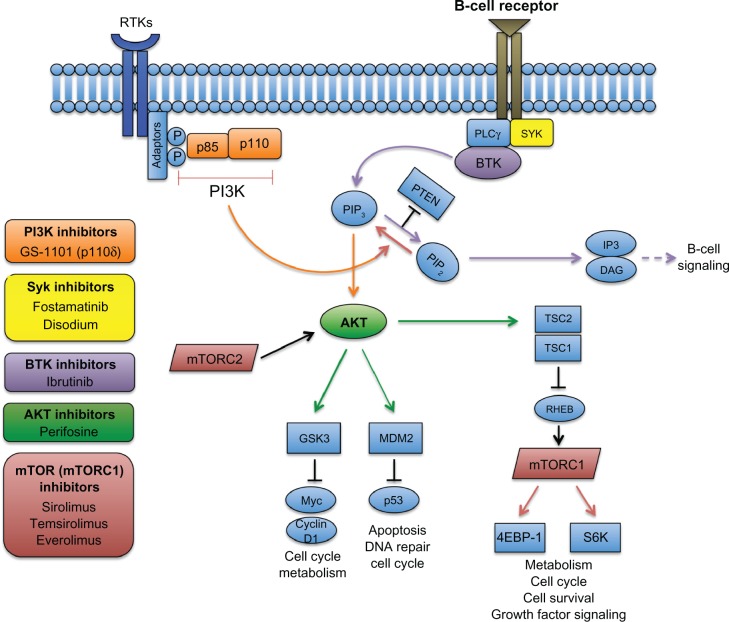
Over the last few decades, advances in immunochemotherapy have led to dramatic improvement in the prognosis of non-Hodgkin's lymphoma (NHL). Despite these advances, relapsed and refractory disease represents a major treatment challenge. For both aggressive and indolent subtypes of NHL, there is no standard of care for salvage regimens, with prognosis after relapse remaining relatively poor. Nevertheless, there are multiple emerging classes of targeted therapies for relapsed/refractory disease, including monoclonal antibodies, antibody- drug conjugates, radioimmunotherapy, small-molecule inhibitors of cell-growth pathways, and novel chemotherapy agents. This review will discuss treatment challenges of NHL, current available salvage regimens for relapsed/refractory NHL, and the safety and efficacy of novel emerging therapies.
Keywords: non-Hodgkin’s lymphoma; novel therapies; relapsed/refractory disease.
Figures
Similar articles
-
[Efficacy of rituximab-containing salvage regimens on relapsed or refractory B-cell non-Hodgkin's lymphoma].Ai Zheng. 2006 Apr;25(4):486-9. Ai Zheng. 2006. PMID: 16613686 Chinese.
-
[Efficacy of GDP regimen (gemcitabine, dexamethasone, and cisplatin) on relapsed or refractory aggressive non-Hodgkin's Lymphoma: a report of 24 cases].Ai Zheng. 2008 Nov;27(11):1222-5. Ai Zheng. 2008. PMID: 19000458 Chinese.
-
Advances in the pathophysiology and treatment of relapsed/refractory Hodgkin's lymphoma with an emphasis on targeted therapies and transplantation strategies.Blood Lymphat Cancer. 2017;7:37-52. doi: 10.2147/BLCTT.S105458. Epub 2017 May 9. Blood Lymphat Cancer. 2017. PMID: 28701859 Free PMC article.
-
Treatment strategies for relapsed and refractory aggressive non-Hodgkin's lymphoma.Expert Opin Pharmacother. 2009 Apr;10(6):983-95. doi: 10.1517/14656560902895715. Expert Opin Pharmacother. 2009. PMID: 19364248 Review.
-
[Salvage therapy in relapsed or refractory malignant lymphoma].Nihon Rinsho. 2000 Mar;58(3):699-703. Nihon Rinsho. 2000. PMID: 10741149 Review. Japanese.
Cited by
-
High-Performance Concurrent Chemo-Immuno-Radiotherapy for the Treatment of Hematologic Cancer through Selective High-Affinity Ligand Antibody Mimic-Functionalized Doxorubicin-Encapsulated Nanoparticles.ACS Cent Sci. 2019 Jan 23;5(1):122-144. doi: 10.1021/acscentsci.8b00746. Epub 2018 Dec 26. ACS Cent Sci. 2019. PMID: 30693332 Free PMC article.
-
Pharmacokinetics of polatuzumab vedotin in combination with R/G-CHP in patients with B-cell non-Hodgkin lymphoma.Cancer Chemother Pharmacol. 2020 May;85(5):831-842. doi: 10.1007/s00280-020-04054-8. Epub 2020 Mar 28. Cancer Chemother Pharmacol. 2020. PMID: 32222808 Free PMC article. Clinical Trial.
-
FDG PET/CT parameters and correlations with tumor-absorbed doses in a phase 1 trial of 177Lu-lilotomab satetraxetan for treatment of relapsed non-Hodgkin lymphoma.Eur J Nucl Med Mol Imaging. 2021 Jun;48(6):1902-1914. doi: 10.1007/s00259-020-05098-x. Epub 2020 Nov 16. Eur J Nucl Med Mol Imaging. 2021. PMID: 33196921 Free PMC article. Clinical Trial.
-
Idelalisib for the treatment of indolent non-Hodgkin lymphoma: a review of its clinical potential.Onco Targets Ther. 2016 May 18;9:2945-53. doi: 10.2147/OTT.S102573. eCollection 2016. Onco Targets Ther. 2016. PMID: 27274288 Free PMC article. Review.
-
Spontaneous Regression of Diffuse Large B-cell Lymphoma in a Patient with Ataxia-Telangiectasia.Adv Biomed Res. 2022 Apr 29;11:31. doi: 10.4103/abr.abr_169_21. eCollection 2022. Adv Biomed Res. 2022. PMID: 35720220 Free PMC article.
References
-
- Zelenetz AD, Abramson JS, Advani RH, et al. NCCN Clinical Practice Guidelines in Oncology: non-Hodgkin’s lymphomas. J Natl Compr Canc Netw. 2010;8(3):288–334. - PubMed
-
- Jaffe ES, Harris NL, Stein H, Vardiman JW, World Health Organization . Classification of Tumours: Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. 3rd ed. Vol. 3. Lyon: IARC; 2001.
-
- Coiffier B, Thieblemont C, Van Den Neste E, et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood. 2010;116(12):2040–2045. - PMC - PubMed
-
- Glennie MJ, French RR, Cragg MS, Taylor RP. Mechanisms of killing by anti-CD20 monoclonal antibodies. Mol Immunol. 2007;44(16):3823–3837. - PubMed
-
- Davis TA, Grillo-López AJ, White CA, et al. Rituximab anti-CD20 monoclonal antibody therapy in non-Hodgkin’s lymphoma: safety and efficacy of re-treatment. J Clin Oncol. 2000;18(17):3135–3143. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
