

Modeling the impact of prevention policies on future diabetes prevalence in the United States: 2010-2030
- PMID: 24047329
- PMCID: PMC3853008
- DOI: 10.1186/1478-7954-11-18
Modeling the impact of prevention policies on future diabetes prevalence in the United States: 2010-2030
Abstract
Background: Although diabetes is one of the most costly and rapidly increasing serious chronic diseases worldwide, the optimal mix of strategies to reduce diabetes prevalence has not been determined.
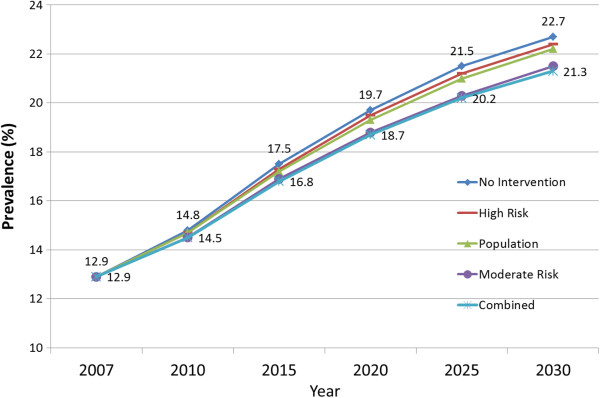
Methods: Using a dynamic model that incorporates national data on diabetes prevalence and incidence, migration, mortality rates, and intervention effectiveness, we project the effect of five hypothetical prevention policies on future US diabetes rates through 2030: 1) no diabetes prevention strategy; 2) a "high-risk" strategy, wherein adults with both impaired fasting glucose (IFG) (fasting plasma glucose of 100-124 mg/dl) and impaired glucose tolerance (IGT) (2-hour post-load glucose of 141-199 mg/dl) receive structured lifestyle intervention; 3) a "moderate-risk" strategy, wherein only adults with IFG are offered structured lifestyle intervention; 4) a "population-wide" strategy, in which the entire population is exposed to broad risk reduction policies; and 5) a "combined" strategy, involving both the moderate-risk and population-wide strategies. We assumed that the moderate- and high-risk strategies reduce the annual diabetes incidence rate in the targeted subpopulations by 12.5% through 2030 and that the population-wide approach would reduce the projected annual diabetes incidence rate by 2% in the entire US population.
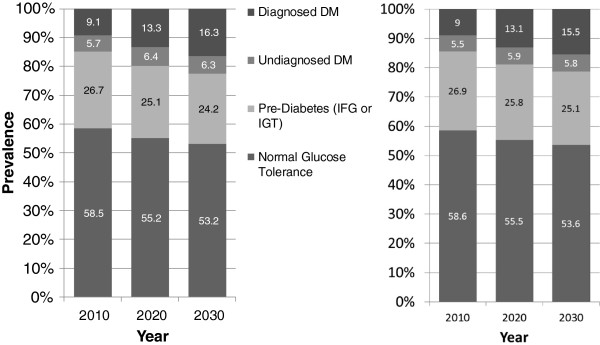
Results: We project that by the year 2030, the combined strategy would prevent 4.6 million incident cases and 3.6 million prevalent cases, attenuating the increase in diabetes prevalence by 14%. The moderate-risk approach is projected to prevent 4.0 million incident cases, 3.1 million prevalent cases, attenuating the increase in prevalence by 12%. The high-risk and population approaches attenuate the projected prevalence increases by 5% and 3%, respectively. Even if the most effective strategy is implemented (the combined strategy), our projections indicate that the diabetes prevalence rate would increase by about 65% over the 23 years (i.e., from 12.9% in 2010 to 21.3% in 2030).
Conclusions: While implementation of appropriate diabetes prevention strategies may slow the rate of increase of the prevalence of diabetes among US adults through 2030, the US diabetes prevalence rate is likely to increase dramatically over the next 20 years. Demand for health care services for people with diabetes complications and diabetes-related disability will continue to grow, and these services will need to be strengthened along with primary diabetes prevention efforts.
Figures
Similar articles
-
Projection of the year 2050 burden of diabetes in the US adult population: dynamic modeling of incidence, mortality, and prediabetes prevalence.Popul Health Metr. 2010 Oct 22;8:29. doi: 10.1186/1478-7954-8-29. Popul Health Metr. 2010. PMID: 20969750 Free PMC article.
-
Impaired glucose tolerance and impaired fasting glycaemia: the current status on definition and intervention.Diabet Med. 2002 Sep;19(9):708-23. doi: 10.1046/j.1464-5491.2002.00835.x. Diabet Med. 2002. PMID: 12207806 Review.
-
Tuberculosis.In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. PMID: 30212088 Free Books & Documents. Review.
-
[Steps toward the primary prevention of type II diabetes mellitus. Various epidemiological considerations].Invest Clin. 1997 Mar;38(1):39-52. Invest Clin. 1997. PMID: 9235072 Review. Spanish.
-
Implications of population growth on prevalence of diabetes. A look at the future.Diabetes Care. 1992 Mar;15 Suppl 1:6-9. doi: 10.2337/diacare.15.1.s6. Diabetes Care. 1992. PMID: 1559424
Cited by
-
Exploring the association between type 2 diabetes and fecal incontinence in american adults: insights from a large cross-sectional study.Int J Colorectal Dis. 2024 Jul 31;39(1):121. doi: 10.1007/s00384-024-04697-6. Int J Colorectal Dis. 2024. PMID: 39085653 Free PMC article.
-
Projection of Diabetes Prevalence in Korean Adults for the Year 2030 Using Risk Factors Identified from National Data.Diabetes Metab J. 2019 Feb;43(1):90-96. doi: 10.4093/dmj.2018.0043. Epub 2018 Oct 31. Diabetes Metab J. 2019. PMID: 30398038 Free PMC article.
-
Racial Disparities in Evidence-Based Management of Metabolic Dysfunction-Associated Steatotic Liver Disease in Patients With Type 2 Diabetes.Endocr Pract. 2024 Jul;30(7):663-669. doi: 10.1016/j.eprac.2024.04.018. Epub 2024 May 1. Endocr Pract. 2024. PMID: 38697305
-
Environmental endocrine disruption of energy metabolism and cardiovascular risk.Curr Diab Rep. 2014 Jun;14(6):494. doi: 10.1007/s11892-014-0494-0. Curr Diab Rep. 2014. PMID: 24756343 Free PMC article. Review.
-
Increased prevalence of cardiac autonomic dysfunction at different degrees of glucose intolerance in the general population: the KORA S4 survey.Diabetologia. 2015 May;58(5):1118-28. doi: 10.1007/s00125-015-3534-7. Epub 2015 Feb 28. Diabetologia. 2015. PMID: 25724570
References
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ. et al.National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378(9785):31–40. doi: 10.1016/S0140-6736(11)60679-X. - DOI - PubMed
-
- Centers for Disease Control and Prevention. National Diabetes Surveillance System. Centers for Disease Control and Prevention. 2008. Available from: URL: http://www.cdc.gov/diabetes/statistics/incidence/fig2.htm.
LinkOut - more resources
Full Text Sources
Other Literature Sources
