

Globular glial tauopathies (GGT): consensus recommendations
- PMID: 23995422
- PMCID: PMC3914659
- DOI: 10.1007/s00401-013-1171-0
Globular glial tauopathies (GGT): consensus recommendations
Abstract
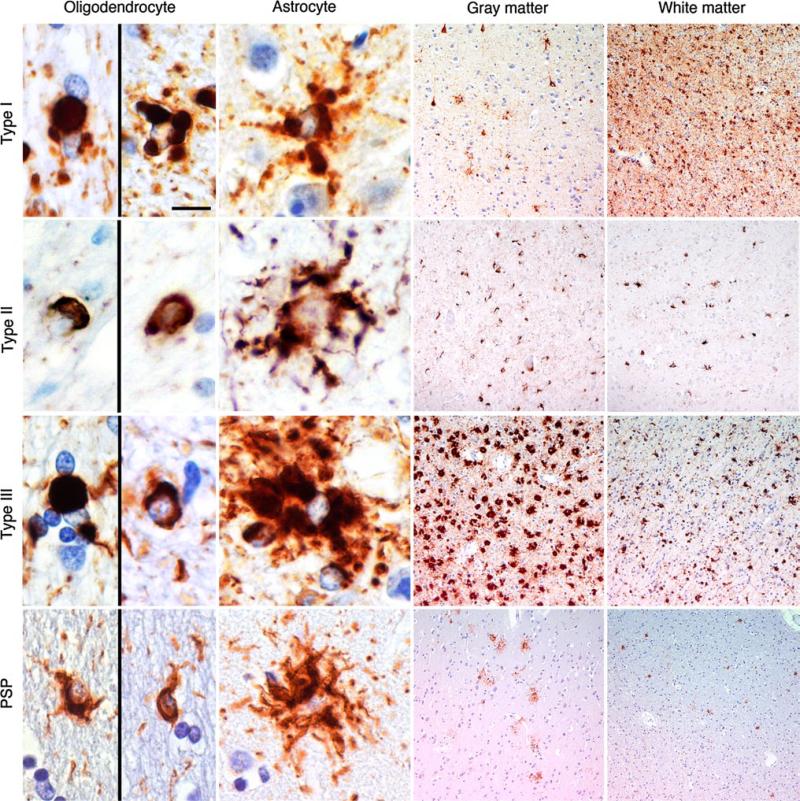
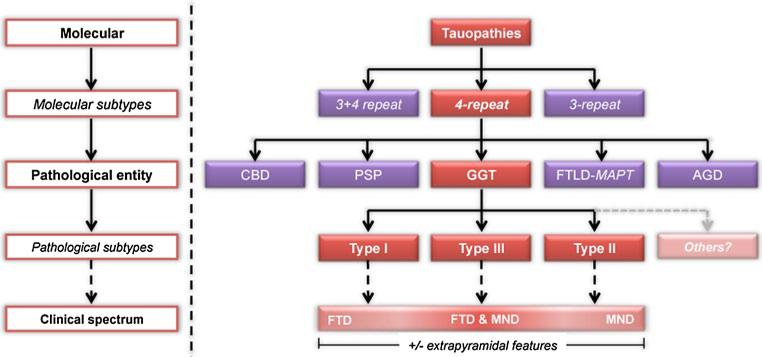
Recent studies have highlighted a group of 4-repeat (4R) tauopathies that are characterised neuropathologically by widespread, globular glial inclusions (GGIs). Tau immunohistochemistry reveals 4R immunoreactive globular oligodendroglial and astrocytic inclusions and the latter are predominantly negative for Gallyas silver staining. These cases are associated with a range of clinical presentations, which correlate with the severity and distribution of underlying tau pathology and neurodegeneration. Their heterogeneous clinicopathological features combined with their rarity and under-recognition have led to cases characterised by GGIs being described in the literature using various and redundant terminologies. In this report, a group of neuropathologists form a consensus on the terminology and classification of cases with GGIs. After studying microscopic images from previously reported cases with suspected GGIs (n = 22), this panel of neuropathologists with extensive experience in the diagnosis of neurodegenerative diseases and a documented record of previous experience with at least one case with GGIs, agreed that (1) GGIs were present in all the cases reviewed; (2) the morphology of globular astrocytic inclusions was different to tufted astrocytes and finally that (3) the cases represented a number of different neuropathological subtypes. They also agreed that the different morphological subtypes are likely to be part of a spectrum of a distinct disease entity, for which they recommend that the overarching term globular glial tauopathy (GGT) should be used. Type I cases typically present with frontotemporal dementia, which correlates with the fronto-temporal distribution of pathology. Type II cases are characterised by pyramidal features reflecting motor cortex involvement and corticospinal tract degeneration. Type III cases can present with a combination of frontotemporal dementia and motor neuron disease with fronto-temporal cortex, motor cortex and corticospinal tract being severely affected. Extrapyramidal features can be present in Type II and III cases and significant degeneration of the white matter is a feature of all GGT subtypes. Improved detection and classification will be necessary for the establishment of neuropathological and clinical diagnostic research criteria in the future.
Figures
Similar articles
-
Globular glial tauopathy Type II: Clinicopathological study of two autopsy cases.Neuropathology. 2019 Apr;39(2):111-119. doi: 10.1111/neup.12532. Epub 2019 Jan 15. Neuropathology. 2019. PMID: 30646429
-
Atypical globular glial tauopathy with a combination of types I and II pathology.Neuropathology. 2019 Apr;39(2):127-134. doi: 10.1111/neup.12536. Epub 2019 Feb 5. Neuropathology. 2019. PMID: 30723950
-
Morphological characterisation of glial and neuronal tau pathology in globular glial tauopathy (Types II and III).Neuropathol Appl Neurobiol. 2020 Jun;46(4):344-358. doi: 10.1111/nan.12581. Epub 2019 Nov 6. Neuropathol Appl Neurobiol. 2020. PMID: 31600825
-
Globular glial tauopathy, a newly recognized white matter tauopathy, with depression/anxiety disorder: report and review of classification.Folia Neuropathol. 2021;59(1):98-103. doi: 10.5114/fn.2021.104396. Folia Neuropathol. 2021. PMID: 33969681 Review.
-
Association Between Globular Glial Tauopathies and Frontotemporal Dementia-Expanding the Spectrum of Gliocentric Disorders: A Review.JAMA Neurol. 2021 Aug 1;78(8):1004-1014. doi: 10.1001/jamaneurol.2021.1813. JAMA Neurol. 2021. PMID: 34152367 Review.
Cited by
-
A molecular pathology, neurobiology, biochemical, genetic and neuroimaging study of progressive apraxia of speech.Nat Commun. 2021 Jun 8;12(1):3452. doi: 10.1038/s41467-021-23687-8. Nat Commun. 2021. PMID: 34103532 Free PMC article. Clinical Trial.
-
Comorbid Neurodegeneration in Primary Progressive Aphasia: Clinicopathological Correlations in a Single-Center Study.Behav Neurol. 2022 Sep 8;2022:6075511. doi: 10.1155/2022/6075511. eCollection 2022. Behav Neurol. 2022. PMID: 36120397 Free PMC article.
-
RNA Binding Proteins and the Pathogenesis of Frontotemporal Lobar Degeneration.Annu Rev Pathol. 2019 Jan 24;14:469-495. doi: 10.1146/annurev-pathmechdis-012418-012955. Epub 2018 Oct 24. Annu Rev Pathol. 2019. PMID: 30355151 Free PMC article. Review.
-
[Tauopathies : From molecule to therapy].Nervenarzt. 2018 Oct;89(10):1083-1094. doi: 10.1007/s00115-018-0584-3. Nervenarzt. 2018. PMID: 30120488 German.
-
Involvement of Oligodendrocytes in Tau Seeding and Spreading in Tauopathies.Front Aging Neurosci. 2019 May 28;11:112. doi: 10.3389/fnagi.2019.00112. eCollection 2019. Front Aging Neurosci. 2019. PMID: 31191295 Free PMC article.
References
-
- Ahmed Z, Doherty KM, Silveira-Moriyama L, et al. Globular glial tauopathies (GGT) presenting with motor neuron disease or frontotemporal dementia: an emerging group of 4-repeat tauopathies. Acta Neuropathol. 2011;122:415–428. - PubMed
-
- Berry RW, Quinn B, Johnson N, Cochran EJ, Ghoshal N, Binder LI. Pathological glial tau accumulations in neurodegenerative disease: review and case report. Neurochem Int. 2001;39:469–479. - PubMed
-
- Bigio EH, Lipton AM, Yen SH, et al. Frontal lobe dementia with novel tauopathy: sporadic multiple system tauopathy with dementia. J Neuropathol Exp Neurol. 2001;60:328–341. - PubMed
-
- Cairns NJ, Atkinson PF, Hanger DP, Anderton BH, Daniel SE, Lantos PL. Tau protein in the glial cytoplasmic inclusions of multiple system atrophy can be distinguished from abnormal tau in Alzheimer's disease. Neurosci Lett. 1997;230:49–52. - PubMed
-
- Dickson DW, Hauw JJ, Agid Y, Litvan I. Progressive supranuclear palsy and corticobasal degeneration. In: Dickson DW, Weller RO, editors. Neurodegeneration: The molecular pathology of dementia and movement disorders. 2nd edn. Wiley-Blackwell; Chichester, West Sussex: 2011. pp. 135–155.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
