

Cerebral extracellular lactate increase is predominantly nonischemic in patients with severe traumatic brain injury
- PMID: 23963367
- PMCID: PMC3824185
- DOI: 10.1038/jcbfm.2013.142
Cerebral extracellular lactate increase is predominantly nonischemic in patients with severe traumatic brain injury
Abstract
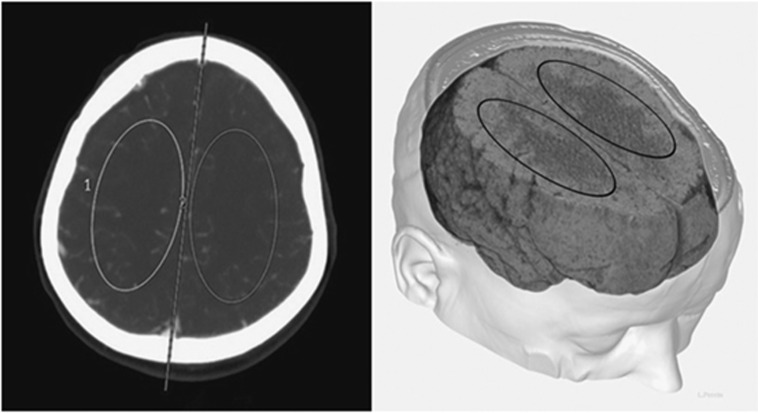
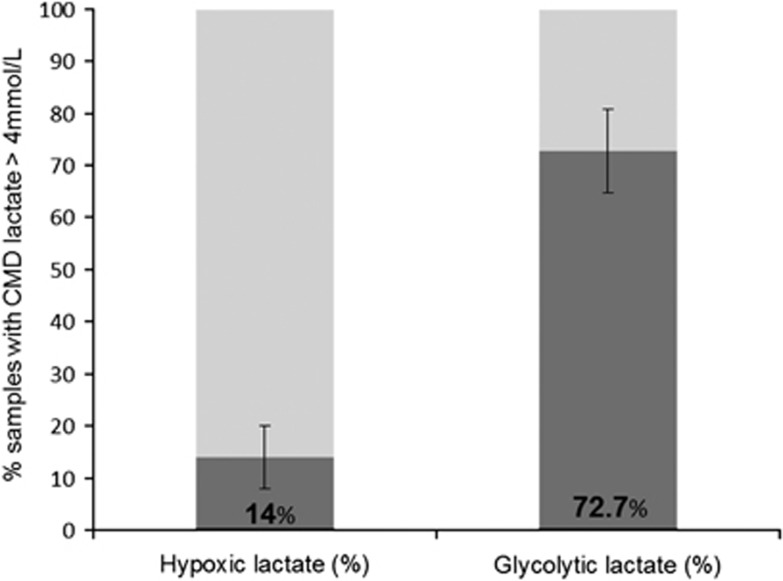
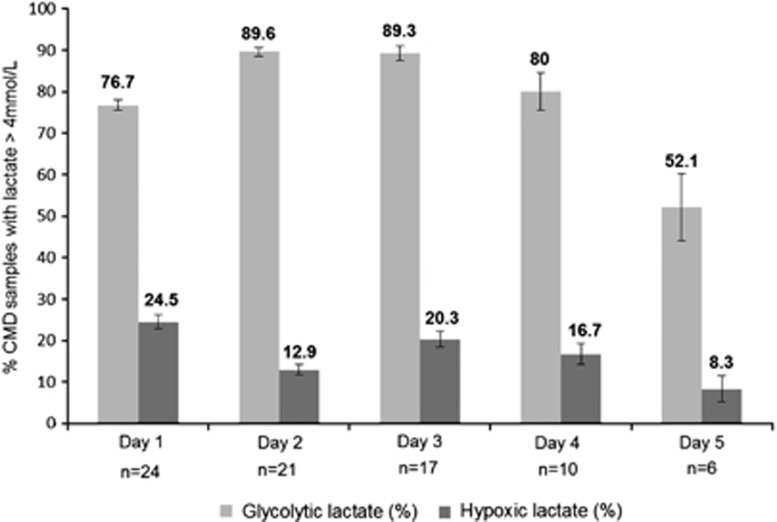
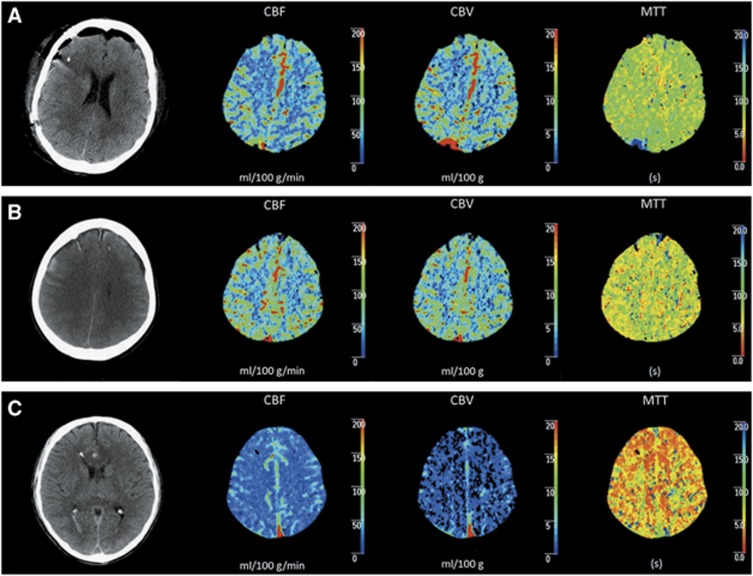
Growing evidence suggests that endogenous lactate is an important substrate for neurons. This study aimed to examine cerebral lactate metabolism and its relationship with brain perfusion in patients with severe traumatic brain injury (TBI). A prospective cohort of 24 patients with severe TBI monitored with cerebral microdialysis (CMD) and brain tissue oxygen tension (PbtO2) was studied. Brain lactate metabolism was assessed by quantification of elevated CMD lactate samples (>4 mmol/L); these were matched to CMD pyruvate and PbtO2 values and dichotomized as glycolytic (CMD pyruvate >119 μmol/L vs. low pyruvate) and hypoxic (PbtO2 <20 mm Hg vs. nonhypoxic). Using perfusion computed tomography (CT), brain perfusion was categorized as oligemic, normal, or hyperemic, and was compared with CMD and PbtO2 data. Samples with elevated CMD lactate were frequently observed (41±8%), and we found that brain lactate elevations were predominantly associated with glycolysis and normal PbtO2 (73±8%) rather than brain hypoxia (14±6%). Furthermore, glycolytic lactate was always associated with normal or hyperemic brain perfusion, whereas all episodes with hypoxic lactate were associated with diffuse oligemia. Our findings suggest predominant nonischemic cerebral extracellular lactate release after TBI and support the concept that lactate may be used as an energy substrate by the injured human brain.
Figures
Similar articles
-
A Prospective Observational Feasibility Study of Jugular Bulb Microdialysis in Subarachnoid Hemorrhage.Neurocrit Care. 2020 Aug;33(1):241-255. doi: 10.1007/s12028-019-00888-0. Neurocrit Care. 2020. PMID: 31845174
-
Accuracy of brain multimodal monitoring to detect cerebral hypoperfusion after traumatic brain injury*.Crit Care Med. 2015 Feb;43(2):445-52. doi: 10.1097/CCM.0000000000000720. Crit Care Med. 2015. PMID: 25393700
-
Protocolized Brain Oxygen Optimization in Subarachnoid Hemorrhage.Neurocrit Care. 2019 Oct;31(2):263-272. doi: 10.1007/s12028-019-00753-0. Neurocrit Care. 2019. PMID: 31218640 Free PMC article.
-
Lactate and the injured brain: friend or foe?Curr Opin Crit Care. 2014 Apr;20(2):133-40. doi: 10.1097/MCC.0000000000000072. Curr Opin Crit Care. 2014. PMID: 24561705 Review.
-
Brain tissue oxygenation, lactate-pyruvate ratio, and cerebrovascular pressure reactivity monitoring in severe traumatic brain injury: systematic review and viewpoint.Neurocrit Care. 2014 Oct;21(2):345-55. doi: 10.1007/s12028-014-0007-7. Neurocrit Care. 2014. PMID: 24993955 Review.
Cited by
-
Lactate in the brain: from metabolic end-product to signalling molecule.Nat Rev Neurosci. 2018 Apr;19(4):235-249. doi: 10.1038/nrn.2018.19. Epub 2018 Mar 8. Nat Rev Neurosci. 2018. PMID: 29515192 Review.
-
Non-Ischemic Cerebral Energy Dysfunction at the Early Brain Injury Phase following Aneurysmal Subarachnoid Hemorrhage.Front Neurol. 2017 Jul 10;8:325. doi: 10.3389/fneur.2017.00325. eCollection 2017. Front Neurol. 2017. PMID: 28740479 Free PMC article.
-
Brain Multimodality Monitoring: Updated Perspectives.Curr Neurol Neurosci Rep. 2016 Jun;16(6):56. doi: 10.1007/s11910-016-0659-0. Curr Neurol Neurosci Rep. 2016. PMID: 27095434 Free PMC article. Review.
-
Glycolysis and the significance of lactate in traumatic brain injury.Front Neurosci. 2015 Apr 8;9:112. doi: 10.3389/fnins.2015.00112. eCollection 2015. Front Neurosci. 2015. PMID: 25904838 Free PMC article. Review.
-
A Precision Medicine Agenda in Traumatic Brain Injury.Front Pharmacol. 2022 Mar 16;13:713100. doi: 10.3389/fphar.2022.713100. eCollection 2022. Front Pharmacol. 2022. PMID: 35370671 Free PMC article. Review.
References
-
- Pellerin L, Pellegri G, Bittar PG, Charnay Y, Bouras C, Martin JL, et al. Evidence supporting the existence of an activity-dependent astrocyte–neuron lactate shuttle. Dev Neurosci. 1998;20:291–299. - PubMed
-
- Bouzier-Sore AK, Voisin P, Canioni P, Magistretti PJ, Pellerin L. Lactate is a preferential oxidative energy substrate over glucose for neurons in culture. J Cereb Blood Flow Metab. 2003;23:1298–1306. - PubMed
-
- Schurr A, Payne RS, Miller JJ, Rigor BM. Brain lactate, not glucose, fuels the recovery of synaptic function from hypoxia upon reoxygenation—an in vitro study. Brain Res. 1997;744:105–111. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
