

Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: a descriptive study
- PMID: 23891402
- PMCID: PMC7185445
- DOI: 10.1016/S1473-3099(13)70204-4
Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: a descriptive study
Abstract
Background: Middle East respiratory syndrome (MERS) is a new human disease caused by a novel coronavirus (CoV). Clinical data on MERS-CoV infections are scarce. We report epidemiological, demographic, clinical, and laboratory characteristics of 47 cases of MERS-CoV infections, identify knowledge gaps, and define research priorities.
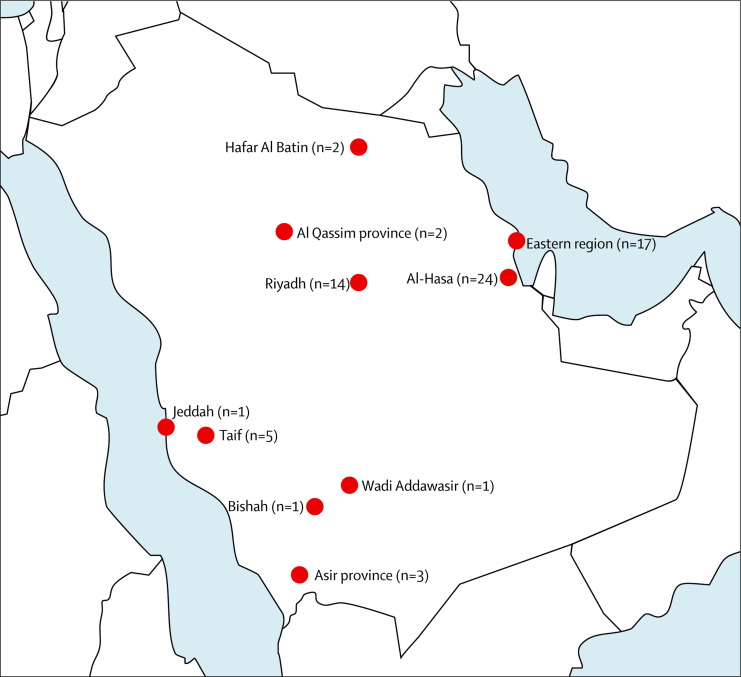
Methods: We abstracted and analysed epidemiological, demographic, clinical, and laboratory data from confirmed cases of sporadic, household, community, and health-care-associated MERS-CoV infections reported from Saudi Arabia between Sept 1, 2012, and June 15, 2013. Cases were confirmed as having MERS-CoV by real-time RT-PCR.
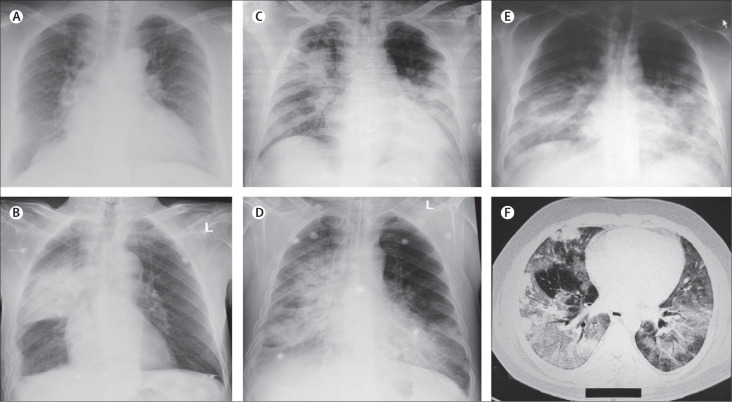
Findings: 47 individuals (46 adults, one child) with laboratory-confirmed MERS-CoV disease were identified; 36 (77%) were male (male:female ratio 3·3:1). 28 patients died, a 60% case-fatality rate. The case-fatality rate rose with increasing age. Only two of the 47 cases were previously healthy; most patients (45 [96%]) had underlying comorbid medical disorders, including diabetes (32 [68%]), hypertension (16 [34%]), chronic cardiac disease (13 [28%]), and chronic renal disease (23 [49%]). Common symptoms at presentation were fever (46 [98%]), fever with chills or rigors (41 [87%]), cough (39 [83%]), shortness of breath (34 [72%]), and myalgia (15 [32%]). Gastrointestinal symptoms were also frequent, including diarrhoea (12 [26%]), vomiting (ten [21%]), and abdominal pain (eight [17%]). All patients had abnormal findings on chest radiography, ranging from subtle to extensive unilateral and bilateral abnormalities. Laboratory analyses showed raised concentrations of lactate dehydrogenase (23 [49%]) and aspartate aminotransferase (seven [15%]) and thrombocytopenia (17 [36%]) and lymphopenia (16 [34%]).
Interpretation: Disease caused by MERS-CoV presents with a wide range of clinical manifestations and is associated with substantial mortality in admitted patients who have medical comorbidities. Major gaps in our knowledge of the epidemiology, community prevalence, and clinical spectrum of infection and disease need urgent definition.
Funding: None.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Is MERS another SARS?Lancet Infect Dis. 2013 Sep;13(9):727-8. doi: 10.1016/S1473-3099(13)70159-2. Epub 2013 Jul 26. Lancet Infect Dis. 2013. PMID: 23891403 Free PMC article. No abstract available.
-
Predicting the potential for within-flight transmission and global dissemination of MERS.Lancet Infect Dis. 2014 Feb;14(2):99. doi: 10.1016/S1473-3099(13)70358-X. Lancet Infect Dis. 2014. PMID: 24457166 Free PMC article. No abstract available.
Similar articles
-
Outbreak of Middle East respiratory syndrome coronavirus in Saudi Arabia: a retrospective study.BMC Infect Dis. 2017 Jan 5;17(1):23. doi: 10.1186/s12879-016-2137-3. BMC Infect Dis. 2017. PMID: 28056850 Free PMC article.
-
Clinical Characteristics and Outcome of Hospitalized COVID-19 Patients in a MERS-CoV Endemic Area.J Epidemiol Glob Health. 2020 Sep;10(3):214-221. doi: 10.2991/jegh.k.200806.002. J Epidemiol Glob Health. 2020. PMID: 32954712 Free PMC article.
-
Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infection: epidemiology, pathogenesis and clinical characteristics.Eur Rev Med Pharmacol Sci. 2018 Aug;22(15):4956-4961. doi: 10.26355/eurrev_201808_15635. Eur Rev Med Pharmacol Sci. 2018. PMID: 30070331
-
Middle East respiratory syndrome coronavirus: risk factors and determinants of primary, household, and nosocomial transmission.Lancet Infect Dis. 2018 Aug;18(8):e217-e227. doi: 10.1016/S1473-3099(18)30127-0. Epub 2018 Apr 18. Lancet Infect Dis. 2018. PMID: 29680581 Free PMC article. Review.
-
Middle East respiratory syndrome coronavirus: implications for health care facilities.Am J Infect Control. 2014 Dec;42(12):1261-5. doi: 10.1016/j.ajic.2014.06.019. Epub 2014 Nov 25. Am J Infect Control. 2014. PMID: 25465253 Free PMC article. Review.
Cited by
-
Pulmonary and Extra-Pulmonary Clinical Manifestations of COVID-19.Front Med (Lausanne). 2020 Aug 13;7:526. doi: 10.3389/fmed.2020.00526. eCollection 2020. Front Med (Lausanne). 2020. PMID: 32903492 Free PMC article. Review.
-
Inhibition of SARS-CoV-2 3CL Mpro by Natural and Synthetic Inhibitors: Potential Implication for Vaccine Production Against COVID-19.Front Mol Biosci. 2021 Apr 12;8:640819. doi: 10.3389/fmolb.2021.640819. eCollection 2021. Front Mol Biosci. 2021. PMID: 33912587 Free PMC article.
-
Development of a novel risk score for the prediction of critical illness amongst COVID-19 patients.Int J Clin Pract. 2021 Apr;75(4):e13915. doi: 10.1111/ijcp.13915. Epub 2020 Dec 22. Int J Clin Pract. 2021. PMID: 33969593 Free PMC article.
-
COVID 19 and liver: An A-Z literature review.Dig Liver Dis. 2021 Feb;53(2):146-152. doi: 10.1016/j.dld.2020.09.010. Epub 2020 Sep 16. Dig Liver Dis. 2021. PMID: 32988758 Free PMC article. Review.
-
Preliminary study to identify severe from moderate cases of COVID-19 using combined hematology parameters.Ann Transl Med. 2020 May;8(9):593. doi: 10.21037/atm-20-3391. Ann Transl Med. 2020. PMID: 32566620 Free PMC article.
References
-
- Centers for Disease Control and Prevention (CDC) Severe respiratory illness associated with a novel coronavirus: Saudi Arabia and Qatar, 2012. MMWR Morb Mortal Wkly Rep. 2012;61:820. - PubMed
-
- Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367:1814–1820. - PubMed
-
- WHO Global alert and response (GAR): Middle East respiratory syndrome coronavirus (MERS-CoV)—update. June 7, 2013. http://www.who.int/csr/don/2013_06_07/en/index.html (accessed June 11, 2013).
-
- WHO Global alert and response (GAR): novel coronavirus summary and literature update. May 17, 2013. http://www.who.int/csr/disease/coronavirus_infections/update_20130517/en... (accessed July 12, 2013).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
