

Cardiovascular risk in rheumatoid arthritis: comparing TNF-α blockade with nonbiologic DMARDs
- PMID: 23885678
- PMCID: PMC4674813
- DOI: 10.1016/j.amjmed.2013.02.016
Cardiovascular risk in rheumatoid arthritis: comparing TNF-α blockade with nonbiologic DMARDs
Abstract
Background: Elevated tumor necrosis factor (TNF)-α likely contributes to the excess cardiovascular risk observed in rheumatoid arthritis. We compared the cardiovascular risk in rheumatoid arthritis patients starting a TNF-α blocking agent versus a nonbiologic disease-modifying antirheumatic drug (nbDMARD).
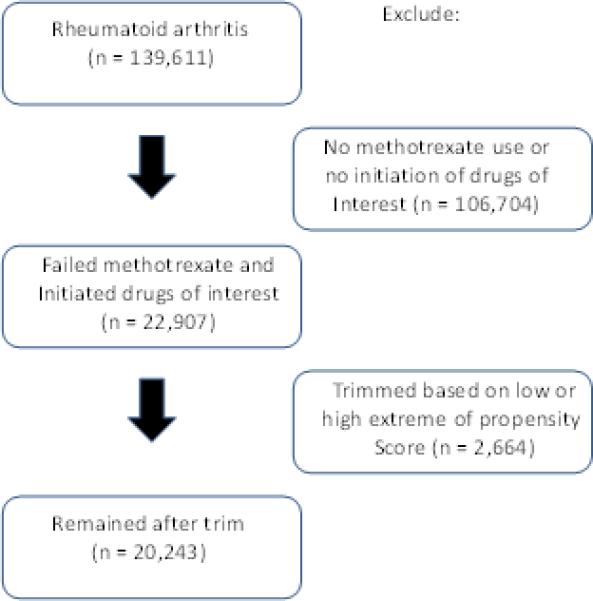
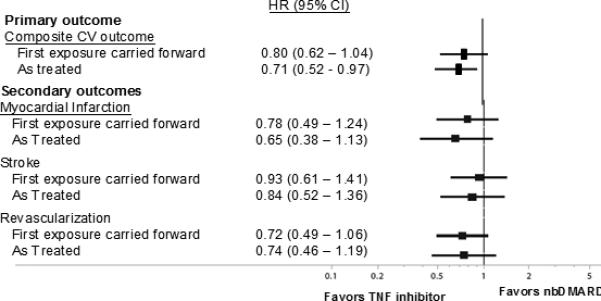
Methods: Subjects with rheumatoid arthritis participating in several different US insurance programs between 1998 and 2007 who received methotrexate were eligible. Those who added a TNF-α blocking agent were compared with subjects who added a nbDMARD in Cox regression models stratified by propensity score decile and adjusted for oral glucocorticoid dosage. We examined the composite cardiovascular end point of myocardial infarction, stroke, or coronary re-vascularization after 6 months.
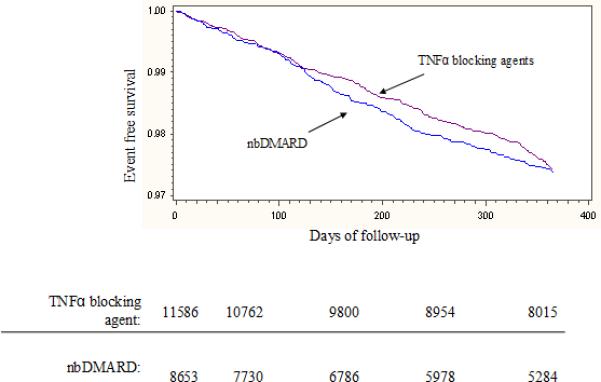
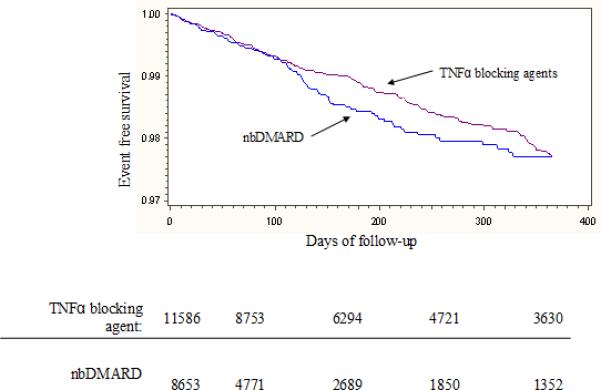
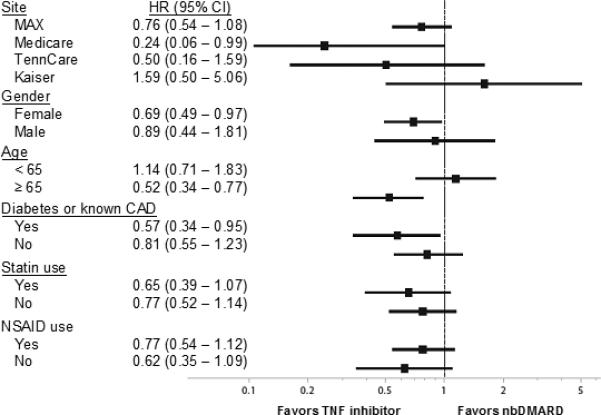
Results: We compared 8656 new users of a nbDMARD with 11,587 new users of a TNF-α blocking agent with similar baseline covariates. Incidence rates per 100 person-years for the composite cardiovascular end point were 3.05 (95% confidence interval [CI], 2.54-3.65) for nbDMARDs and 2.52 (95% CI, 2.12-2.98) for TNF-α blocking agents. The hazard ratio (HR) for the TNF-α blocking agent compared with nbDMARD carrying the first exposure forward was 0.80 (95%, CI 0.62-1.04), while the HR for the as-treated analysis was 0.71 (95% CI, 0.52-0.97). The potential cardiovascular benefit of TNF-α blocking agents was strongest among individuals ≥65 years of age (HR 0.52; 95% CI, 0.34 -0.77; P for interaction = 0.075).
Conclusion: Among subjects with rheumatoid arthritis, TNF-α blocking agents may be associated with a reduced risk of cardiovascular events compared with an nbDMARD. Randomized controlled clinical trials should be considered to test this hypothesis.
Keywords: Cardiovascular disease; Rheumatoid arthritis; TNF-α blocking agents.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Heart failure risk among patients with rheumatoid arthritis starting a TNF antagonist.Ann Rheum Dis. 2013 Nov;72(11):1813-8. doi: 10.1136/annrheumdis-2012-202136. Epub 2012 Nov 15. Ann Rheum Dis. 2013. PMID: 23155221
-
The risk of cancer in patients with rheumatoid arthritis taking tumor necrosis factor antagonists: a nationwide cohort study.Arthritis Res Ther. 2014 Sep 30;16(5):449. doi: 10.1186/s13075-014-0449-5. Arthritis Res Ther. 2014. PMID: 25267341 Free PMC article.
-
Tumor Necrosis Factor-α Inhibitor Use and the Risk of Incident Hypertension in Patients with Rheumatoid Arthritis.Epidemiology. 2016 May;27(3):414-22. doi: 10.1097/EDE.0000000000000446. Epidemiology. 2016. PMID: 26808597 Free PMC article.
-
Comparison of the efficacy of the tumour necrosis factor alpha blocking agents adalimumab, etanercept, and infliximab when added to methotrexate in patients with active rheumatoid arthritis.Ann Rheum Dis. 2003 Nov;62 Suppl 2(Suppl 2):ii13-6. doi: 10.1136/ard.62.suppl_2.ii13. Ann Rheum Dis. 2003. PMID: 14532140 Free PMC article. Review.
-
Rheumatoid arthritis: choice of antirheumatic treatment. Methotrexate first.Prescrire Int. 2010 Feb;19(105):30-4. Prescrire Int. 2010. PMID: 20455343 Review.
Cited by
-
Metabolic Abnormalities, Cardiovascular Disease, and Metabolic Syndrome in Adult Rheumatoid Arthritis Patients: Current Perspectives and Clinical Implications.Open Access Rheumatol. 2022 Nov 4;14:255-267. doi: 10.2147/OARRR.S285407. eCollection 2022. Open Access Rheumatol. 2022. PMID: 36388145 Free PMC article. Review.
-
Increased cardiovascular risk in rheumatoid arthritis: mechanisms and implications.BMJ. 2018 Apr 23;361:k1036. doi: 10.1136/bmj.k1036. BMJ. 2018. PMID: 29685876 Free PMC article. Review.
-
[Treatment of cardiovascular risk factors].Z Rheumatol. 2016 Mar;75(2):173-80; quiz 181-2. doi: 10.1007/s00393-016-0064-8. Z Rheumatol. 2016. PMID: 26924198 German.
-
Epicardial fat thickness as cardiovascular risk factor and therapeutic target in patients with rheumatoid arthritis treated with biological and nonbiological therapies.Arthritis. 2014;2014:782850. doi: 10.1155/2014/782850. Epub 2014 Dec 10. Arthritis. 2014. PMID: 25574390 Free PMC article.
-
Dissolving microneedle patch-assisted transdermal delivery of methotrexate improve the therapeutic efficacy of rheumatoid arthritis.Drug Deliv. 2023 Dec;30(1):121-132. doi: 10.1080/10717544.2022.2157518. Drug Deliv. 2023. PMID: 36533887 Free PMC article.
References
-
- Cesari M, Penninx BW, Newman AB, et al. Inflammatory markers and onset of cardiovascular events: results from the Health ABC study. Circulation. 2003;108(19):2317–22. - PubMed
-
- Ridker PM, Rifai N, Pfeffer M, Sacks F, Lepage S, Braunwald E. Elevation of tumor necrosis factor-alpha and increased risk of recurrent coronary events after myocardial infarction. Circulation. 2000;101(18):2149–53. - PubMed
-
- Lee DM, Weinblatt ME. Rheumatoid arthritis. Lancet. 2001;358(9285):903–11. - PubMed
-
- Feldmann M, Brennan FM, Maini RN. Role of cytokines in rheumatoid arthritis. Annual review of immunology. 1996;14:397–440. - PubMed
-
- Solomon DH, Karlson EW, Rimm EB, et al. Cardiovascular morbidity and mortality in women diagnosed with rheumatoid arthritis.[see comment]. Circulation. 2003;107(9):1303–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
