

doi: 10.2337/dcS13-2008.
Role of reduced β-cell mass versus impaired β-cell function in the pathogenesis of type 2 diabetes
Affiliations
- PMID: 23882035
- PMCID: PMC3920783
- DOI: 10.2337/dcS13-2008
Item in Clipboard
Role of reduced β-cell mass versus impaired β-cell function in the pathogenesis of type 2 diabetes
Diabetes Care.
2013 Aug.
No abstract available
Figures
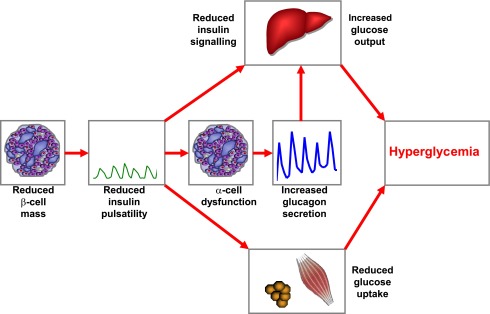
Working model for the impact of reduced β-cell mass on the pathogenesis of type 2 diabetes. In patients with type 2 diabetes, β-cell mass is reduced by ∼20–65%, leading to impaired and delayed insulin secretion and a specific reduction in the amplitude of pulsatile insulin secretion. The reduction of insulin secretion and insulin pulsatility leads to disruption of the intraislet insulin-glucagon cross-talk, causing insufficient suppression of glucagon release. Reduced pulsatile insulin secretion impairs hepatic insulin signaling and perturbs peripheral insulin action. Increased hepatic glucose release is further augmented by the exaggerated glucagon concentrations. Together, these defects cause hyperglycemia in patients with type 2 diabetes.
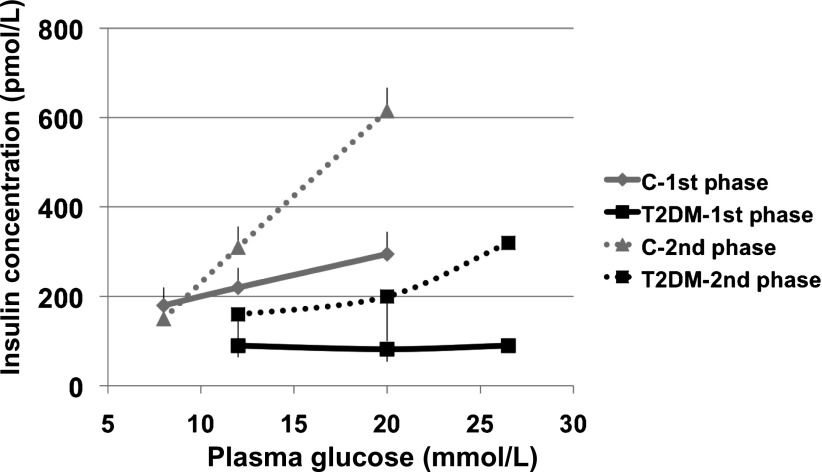
Stimulus response curve for first-phase (derivative control of β-cell function) (continuous lines) and second-phase (proportional control of β-cell function) (dotted lines) insulin release in control subjects (C) and in patients with type 2 diabetes (T2DM). All subjects underwent a number of hyperglycemic clamps at graded glucose levels to construct a stimulus response curve in each. Although both first- and second-phase insulin releases are severely impaired in the patients (P < 0.01 for both, type 2 diabetic vs. control), second phase shows a graded response to the glucose challenge, whereas first phase is virtually absent in the patients, thereby showing asymmetric functional defects. Data are redrawn from ref. .
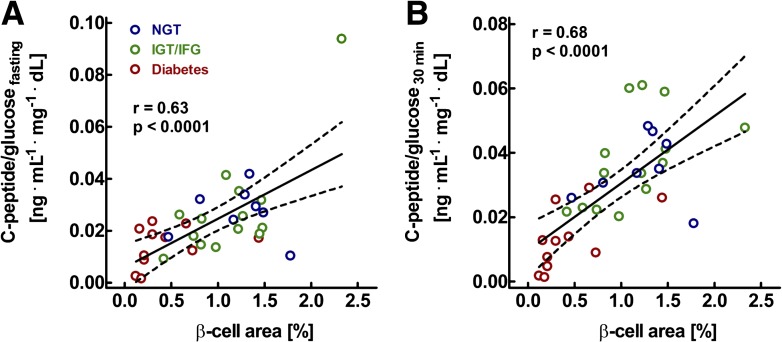
Relationship between pancreatic β-cell area, as determined from pancreatic tissue removed at surgery, and the C-peptide–to–glucose ratio determined in the fasting state (A) and 30 min after oral glucose ingestion in 8 individuals with normal glucose tolerance (NGT), 14 with impaired fasting glucose (IFG) or impaired glucose tolerance (IGT), and 11 with diabetes. r and P values were calculated by linear regression analysis. These analyses demonstrate the tight relationship between β-cell mass and β-cell function. Modified from ref. .
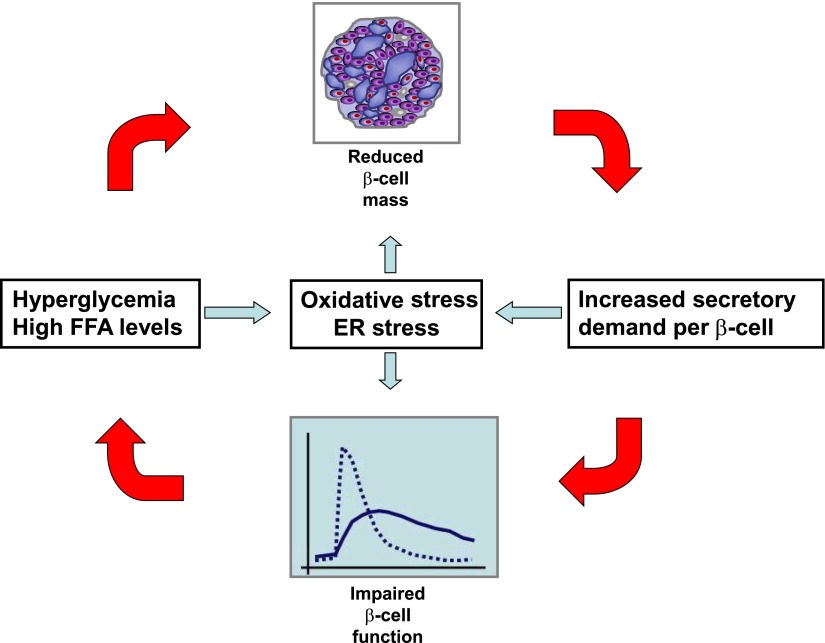
Consensus model for the relationship between impaired β-cell function and mass in type 2 diabetes. A reduction in β-cell mass increases the secretory demand to the remaining β-cells, thereby disturbing β-cell function. This may lead to hyperglycemia and hyperlipidemia, which may again induce β-cell apoptosis, thereby aggravating the β-cell deficit. Along the same lines, the vicious circle may be initiated by a primary defect in β-cell function. The detrimental effects of hyperglycemia and β-cell exhaustion on β-cell mass and function may involve both oxidative stress and ER stress. FFA, free fatty acid.
Similar articles
-
Beta cells in type 2 diabetes - a crucial contribution to pathogenesis.Diabetes Obes Metab. 2008 May;10(5):408-20. doi: 10.1111/j.1463-1326.2007.00718.x. Epub 2007 Apr 19. Diabetes Obes Metab. 2008. PMID: 17451426 Review.
-
Diminished glucagon suppression after β-cell reduction is due to impaired α-cell function rather than an expansion of α-cell mass.Am J Physiol Endocrinol Metab. 2011 Apr;300(4):E717-23. doi: 10.1152/ajpendo.00315.2010. Epub 2011 Feb 1. Am J Physiol Endocrinol Metab. 2011. PMID: 21285404 Free PMC article.
-
The beta cell lesion in type 2 diabetes: there has to be a primary functional abnormality.Diabetologia. 2009 Jun;52(6):1003-12. doi: 10.1007/s00125-009-1321-z. Epub 2009 Mar 27. Diabetologia. 2009. PMID: 19326096 Free PMC article. Review.
-
Insulin resistance versus beta-cell dysfunction in the pathogenesis of type 2 diabetes.Curr Diab Rep. 2009 Jun;9(3):188-9. doi: 10.1007/s11892-009-0031-8. Curr Diab Rep. 2009. PMID: 19490819 No abstract available.
-
Goals of treatment for type 2 diabetes: beta-cell preservation for glycemic control.Diabetes Care. 2009 Nov;32 Suppl 2(Suppl 2):S178-83. doi: 10.2337/dc09-S306. Diabetes Care. 2009. PMID: 19875548 Free PMC article. Review. No abstract available.
Cited by
-
Glucokinase is required for high-starch diet-induced β-cell mass expansion in mice.J Diabetes Investig. 2021 Sep;12(9):1545-1554. doi: 10.1111/jdi.13532. Epub 2021 Mar 30. J Diabetes Investig. 2021. PMID: 33638884 Free PMC article.
-
Loss of Free Fatty Acid Receptor 2 leads to impaired islet mass and beta cell survival.Sci Rep. 2016 Jun 21;6:28159. doi: 10.1038/srep28159. Sci Rep. 2016. PMID: 27324831 Free PMC article.
-
Changing the Concept of Type 2 Diabetes: Beta Cell Workload Hypothesis Revisited.Endocr Metab Immune Disord Drug Targets. 2019;19(2):121-127. doi: 10.2174/1871530318666180821161825. Endocr Metab Immune Disord Drug Targets. 2019. PMID: 30173655 Free PMC article. Review.
-
It's ok to be outnumbered - sub-stoichiometric modulation of homomeric protein complexes.RSC Med Chem. 2022 Oct 27;14(1):22-46. doi: 10.1039/d2md00212d. eCollection 2023 Jan 25. RSC Med Chem. 2022. PMID: 36760737 Free PMC article. Review.
-
Does disruption of circadian rhythms contribute to beta-cell failure in type 2 diabetes?Curr Diab Rep. 2014 Apr;14(4):474. doi: 10.1007/s11892-014-0474-4. Curr Diab Rep. 2014. PMID: 24532160 Free PMC article. Review.
References
-
- DeFronzo RA. Pathogenesis of type 2 (non-insulin dependent) diabetes mellitus: a balanced overview. Diabetologia 1992;35:389–397 - PubMed
-
- Pfeifer MA, Halter JB, Porte D., Jr Insulin secretion in diabetes mellitus. Am J Med 1981;70:579–588 - PubMed
-
- Meigs JB, Wilson PW, Fox CS, et al. Body mass index, metabolic syndrome, and risk of type 2 diabetes or cardiovascular disease. J Clin Endocrinol Metab 2006;91:2906–2912 - PubMed
-
- Klöppel G, Löhr M, Habich K, Oberholzer M, Heitz PU. Islet pathology and the pathogenesis of type 1 and type 2 diabetes mellitus revisited. Surv Synth Pathol Res 1985;4:110–125 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
