

Interhuman transmissibility of Middle East respiratory syndrome coronavirus: estimation of pandemic risk
- PMID: 23831141
- PMCID: PMC7159280
- DOI: 10.1016/S0140-6736(13)61492-0
Interhuman transmissibility of Middle East respiratory syndrome coronavirus: estimation of pandemic risk
Abstract
Background: The new Middle East respiratory syndrome coronavirus (MERS-CoV) infection shares many clinical, epidemiological, and virological similarities with that of severe acute respiratory syndrome (SARS)-CoV. We aimed to estimate virus transmissibility and the epidemic potential of MERS-CoV, and to compare the results with similar findings obtained for prepandemic SARS.
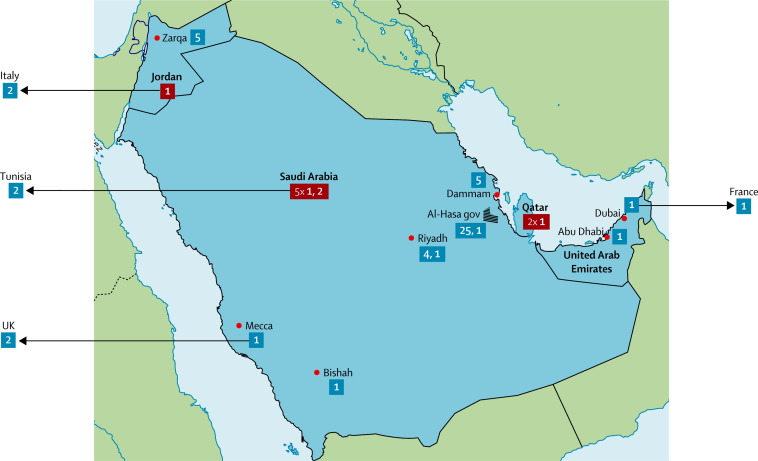
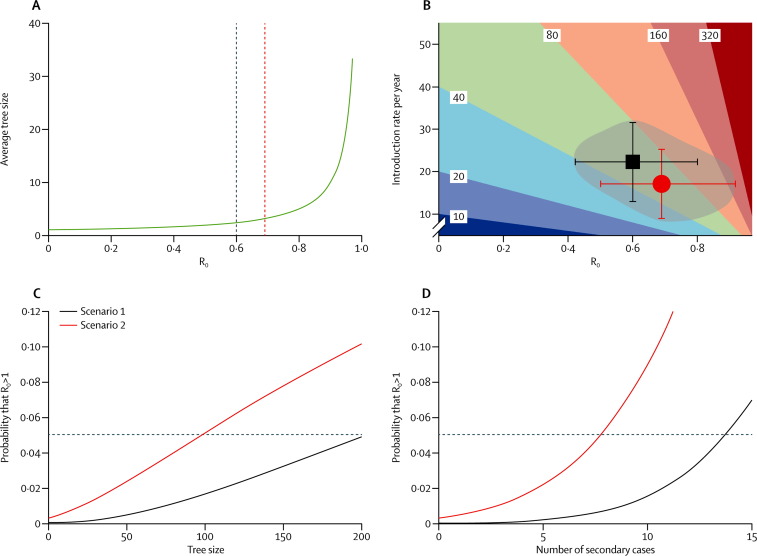
Methods: We retrieved data for MERS-CoV clusters from the WHO summary and subsequent reports, and published descriptions of cases, and took into account 55 of the 64 laboratory-confirmed cases of MERS-CoV reported as of June 21, 2013, excluding cases notified in the previous 2 weeks. To assess the interhuman transmissibility of MERS-CoV, we used Bayesian analysis to estimate the basic reproduction number (R0) and compared it to that of prepandemic SARS. We considered two scenarios, depending on the interpretation of the MERS-CoV cluster-size data.
Results: With our most pessimistic scenario (scenario 2), we estimated MERS-CoV R0 to be 0·69 (95% CI 0·50-0·92); by contrast, the R0 for prepandemic SARS-CoV was 0·80 (0·54-1·13). Our optimistic scenario (scenario 1) yielded a MERS-CoV R0 of 0·60 (0·42-0·80). Because of recent implementation of effective contact tracing and isolation procedures, further MERS-CoV transmission data might no longer describe an entire cluster, but only secondary infections directly caused by the index patient. Hence, we calculated that, under scenario 2, eight or more secondary infections caused by the next index patient would translate into a 5% or higher chance that the revised MERS-CoV R0 would exceed 1--ie, that MERS-CoV might have pandemic potential.
Interpretation: Our analysis suggests that MERS-CoV does not yet have pandemic potential. We recommend enhanced surveillance, active contact tracing, and vigorous searches for the MERS-CoV animal hosts and transmission routes to human beings.
Funding: Agence Nationale de la Recherche (Labex Integrative Biology of Emerging Infectious Diseases), and the European Community's Seventh Framework Programme project PREDEMICS.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Assessing the pandemic potential of MERS-CoV.Lancet. 2013 Aug 24;382(9893):662-4. doi: 10.1016/S0140-6736(13)61504-4. Epub 2013 Jul 5. Lancet. 2013. PMID: 23831143 Free PMC article. No abstract available.
Similar articles
-
Middle East respiratory syndrome coronavirus: quantification of the extent of the epidemic, surveillance biases, and transmissibility.Lancet Infect Dis. 2014 Jan;14(1):50-56. doi: 10.1016/S1473-3099(13)70304-9. Epub 2013 Nov 13. Lancet Infect Dis. 2014. PMID: 24239323 Free PMC article.
-
Clinical features and viral diagnosis of two cases of infection with Middle East Respiratory Syndrome coronavirus: a report of nosocomial transmission.Lancet. 2013 Jun 29;381(9885):2265-72. doi: 10.1016/S0140-6736(13)60982-4. Epub 2013 May 30. Lancet. 2013. PMID: 23727167 Free PMC article.
-
Coronaviruses: severe acute respiratory syndrome coronavirus and Middle East respiratory syndrome coronavirus in travelers.Curr Opin Infect Dis. 2014 Oct;27(5):411-7. doi: 10.1097/QCO.0000000000000089. Curr Opin Infect Dis. 2014. PMID: 25033169 Review.
-
Middle East respiratory syndrome.Lancet. 2015 Sep 5;386(9997):995-1007. doi: 10.1016/S0140-6736(15)60454-8. Epub 2015 Jun 3. Lancet. 2015. PMID: 26049252 Free PMC article. Review.
-
The discrepant epidemiology of Middle East respiratory syndrome coronavirus (MERS-CoV).Environ Syst Decis. 2014;34(3):383-390. doi: 10.1007/s10669-014-9506-5. Epub 2014 Jul 25. Environ Syst Decis. 2014. PMID: 32288979 Free PMC article.
Cited by
-
Assessing the pandemic potential of MERS-CoV.Lancet. 2013 Aug 24;382(9893):662-4. doi: 10.1016/S0140-6736(13)61504-4. Epub 2013 Jul 5. Lancet. 2013. PMID: 23831143 Free PMC article. No abstract available.
-
Using the Pillars of Infection Prevention to Build an Effective Program for Reducing the Transmission of Emerging and Reemerging Infections.Curr Environ Health Rep. 2015 Sep;2(3):226-35. doi: 10.1007/s40572-015-0059-7. Curr Environ Health Rep. 2015. PMID: 26231500 Free PMC article.
-
Nosocomial infection control in healthcare settings: Protection against emerging infectious diseases.Infect Dis Poverty. 2016 Apr 12;5:30. doi: 10.1186/s40249-016-0118-9. Infect Dis Poverty. 2016. PMID: 27068809 Free PMC article.
-
Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: a descriptive study.Lancet Infect Dis. 2013 Sep;13(9):752-61. doi: 10.1016/S1473-3099(13)70204-4. Epub 2013 Jul 26. Lancet Infect Dis. 2013. PMID: 23891402 Free PMC article.
-
A comparative overview of COVID-19, MERS and SARS: Review article.Int J Surg. 2020 Sep;81:1-8. doi: 10.1016/j.ijsu.2020.07.032. Epub 2020 Jul 26. Int J Surg. 2020. PMID: 32730205 Free PMC article. Review.
References
-
- WHO MERS-CoV summary and literature update—as of 20 June 2013. http://www.who.int/csr/disease/coronavirus_infections/update_20130620 (accessed June 24, 2013).
-
- Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus ADME, Fouchier RAM. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367:1814–1820. - PubMed
-
- Health Protection Agency (HPA) UK Novel Coronavirus Investigation team Evidence of person-to-person transmission within a family cluster of novel coronavirus infections, United Kingdom, February 2013. Euro Surveill. 2013;18:20427. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
