

Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association
- PMID: 23616602
- PMCID: PMC3908895
- DOI: 10.1161/HHF.0b013e318291329a
Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association
Abstract
Background: Heart failure (HF) is an important contributor to both the burden and cost of national healthcare expenditures, with more older Americans hospitalized for HF than for any other medical condition. With the aging of the population, the impact of HF is expected to increase substantially.
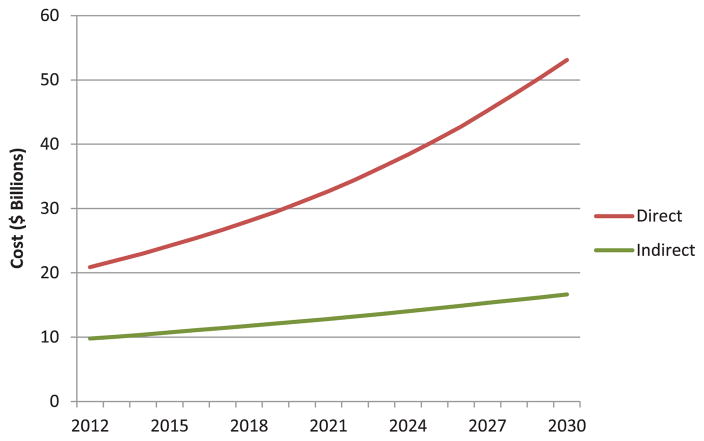
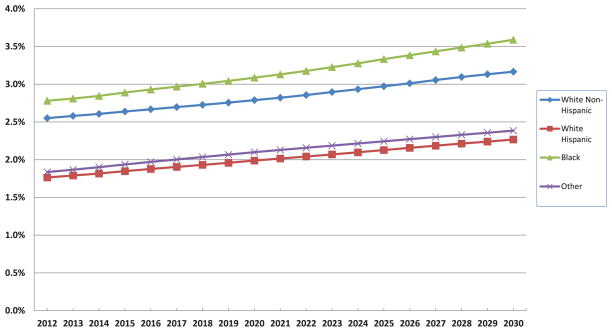
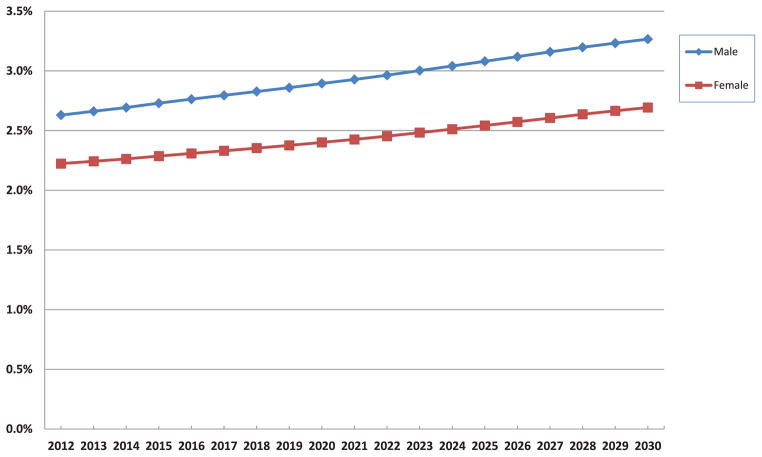
Methods and results: We estimated future costs of HF by adapting a methodology developed by the American Heart Association to project the epidemiology and future costs of HF from 2012 to 2030 without double counting the costs attributed to comorbid conditions. The model assumes that HF prevalence will remain constant by age, sex, and race/ethnicity and that rising costs and technological innovation will continue at the same rate. By 2030, >8 million people in the United States (1 in every 33) will have HF. Between 2012 and 2030, real (2010$) total direct medical costs of HF are projected to increase from $21 billion to $53 billion. Total costs, including indirect costs for HF, are estimated to increase from $31 billion in 2012 to $70 billion in 2030. If one assumes all costs of cardiac care for HF patients are attributable to HF (no cost attribution to comorbid conditions), the 2030 projected cost estimates of treating patients with HF will be 3-fold higher ($160 billion in direct costs).
Conclusions: The estimated prevalence and cost of care for HF will increase markedly because of aging of the population. Strategies to prevent HF and improve the efficiency of care are needed.
Keywords: AHA Scientific Statements; heart failure.
Figures
Similar articles
-
Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association.Circulation. 2011 Mar 1;123(8):933-44. doi: 10.1161/CIR.0b013e31820a55f5. Epub 2011 Jan 24. Circulation. 2011. PMID: 21262990
-
Projected Costs of Informal Caregiving for Cardiovascular Disease: 2015 to 2035: A Policy Statement From the American Heart Association.Circulation. 2018 May 8;137(19):e558-e577. doi: 10.1161/CIR.0000000000000570. Epub 2018 Apr 9. Circulation. 2018. PMID: 29632217 Review.
-
Forecasting the future of stroke in the United States: a policy statement from the American Heart Association and American Stroke Association.Stroke. 2013 Aug;44(8):2361-75. doi: 10.1161/STR.0b013e31829734f2. Epub 2013 May 22. Stroke. 2013. PMID: 23697546
-
Forecasting the Economic Burden of Cardiovascular Disease and Stroke in the United States Through 2050: A Presidential Advisory From the American Heart Association.Circulation. 2024 Jul 23;150(4):e89-e101. doi: 10.1161/CIR.0000000000001258. Epub 2024 Jun 4. Circulation. 2024. PMID: 38832515 Review.
-
National Burden of Heart Failure Events in the United States, 2006 to 2014.Circ Heart Fail. 2018 Dec;11(12):e004873. doi: 10.1161/CIRCHEARTFAILURE.117.004873. Circ Heart Fail. 2018. PMID: 30562099 Free PMC article.
Cited by
-
Association of Medication Adherence and Health Status in Heart Failure With Reduced Ejection Fraction: Insights From the CHAMP-HF Registry.Circ Cardiovasc Qual Outcomes. 2024 Sep;17(9):e010211. doi: 10.1161/CIRCOUTCOMES.123.010211. Epub 2024 Jul 24. Circ Cardiovasc Qual Outcomes. 2024. PMID: 39045701
-
A Robust e-Epidemiology Tool in Phenotyping Heart Failure with Differentiation for Preserved and Reduced Ejection Fraction: the Electronic Medical Records and Genomics (eMERGE) Network.J Cardiovasc Transl Res. 2015 Nov;8(8):475-83. doi: 10.1007/s12265-015-9644-2. Epub 2015 Jul 21. J Cardiovasc Transl Res. 2015. PMID: 26195183 Free PMC article.
-
Health literacy and mortality: a cohort study of patients hospitalized for acute heart failure.J Am Heart Assoc. 2015 Apr 29;4(5):e001799. doi: 10.1161/JAHA.115.001799. J Am Heart Assoc. 2015. PMID: 25926328 Free PMC article.
-
Epigenetics of the failing heart.Heart Fail Rev. 2015 Jul;20(4):435-59. doi: 10.1007/s10741-015-9483-x. Heart Fail Rev. 2015. PMID: 25847519 Review.
-
Investigating changes in disease activity as a mediator of cardiovascular risk reduction with methotrexate use in rheumatoid arthritis.Ann Rheum Dis. 2021 Nov;80(11):1385-1392. doi: 10.1136/annrheumdis-2021-220125. Epub 2021 May 28. Ann Rheum Dis. 2021. PMID: 34049859 Free PMC article.
References
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. . Heart disease and stroke statistics--2012 update: a report from the American Heart Association [published correction appears in Circulation. 2012;125:e1002] Circulation. 2012;125:e2–e220. - PMC - PubMed
-
- Barker WH, Mullooly JP, Getchell W. Changing incidence and survival for heart failure in a well-defined older population, 1970–1974 and 1990–1994. Circulation. 2006;113:799–805. - PubMed
-
- Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD, Finkelstein EA, Hong Y, Johnston SC, Khera A, Lloyd-Jones DM, Nelson SA, Nichol G, Orenstein D, Wilson PW, Woo YJ on behalf of the American Heart Association Advocacy Coordinating Committee, Stroke Council, Council on Cardiovascular Radiology and Intervention Council on Clinical Cardiology, Council on Epidemiology and Prevention Council on Arteriosclerosis, Thrombosis and Vascular Biology, Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation Council on Cardiovascular Nursing, Council on the Kidney in Cardiovascular Disease, Council on Cardiovascular Surgery and Anesthesia, and Interdisciplinary Council on Quality of Care and Outcomes Research. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123:933–944. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
