

Use of selective serotonin reuptake inhibitors and outcomes in pulmonary arterial hypertension
- PMID: 23558791
- PMCID: PMC4694099
- DOI: 10.1378/chest.12-2081
Use of selective serotonin reuptake inhibitors and outcomes in pulmonary arterial hypertension
Abstract
Background: Selective serotonin reuptake inhibitors (SSRIs) have been suggested to offer therapeutic benefit in patients with pulmonary arterial hypertension (PAH). We conducted two analyses to explore the association between SSRI use and PAH outcomes using the Registry to Evaluate Early and Long-term PAH Disease Management (REVEAL Registry).
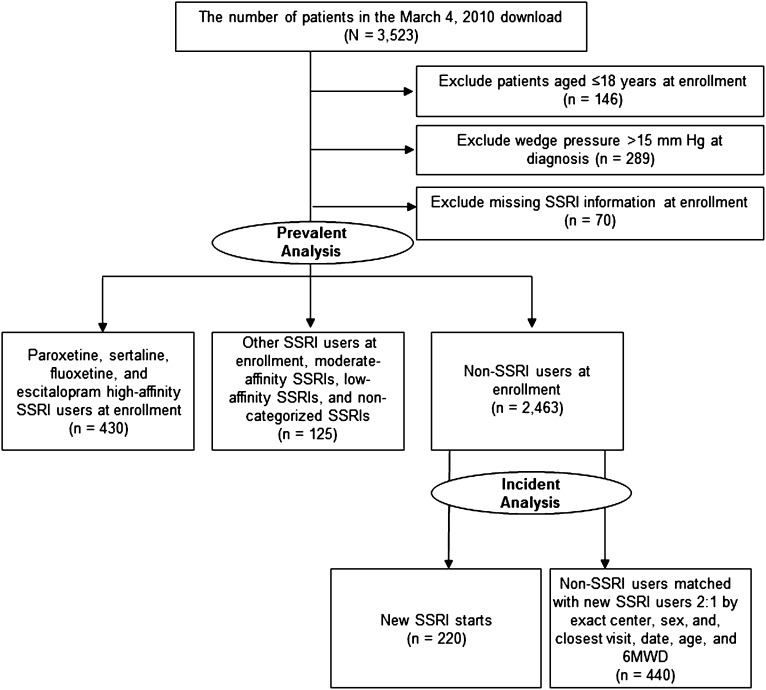
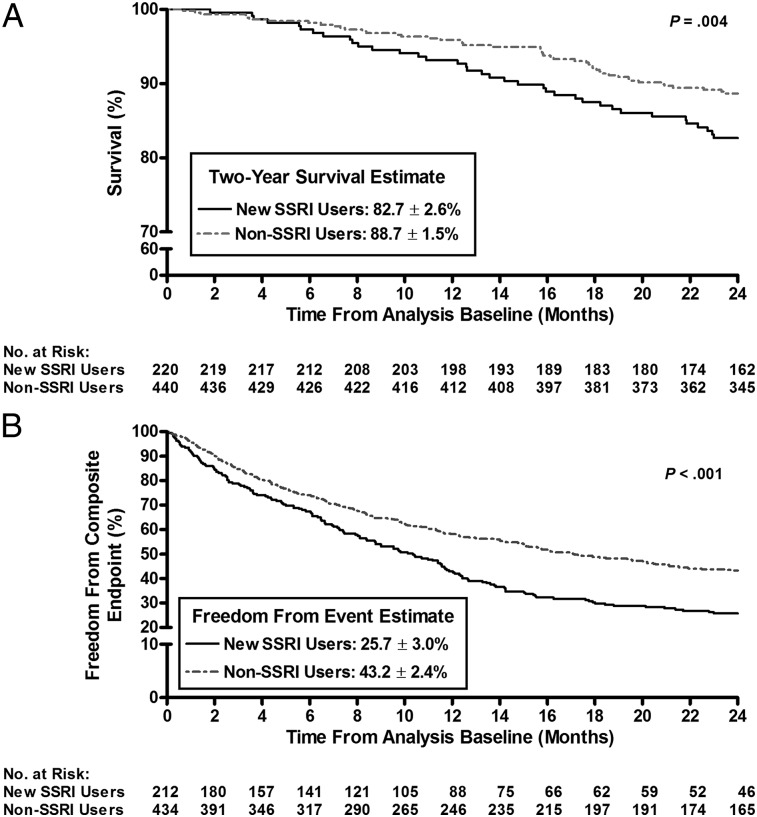
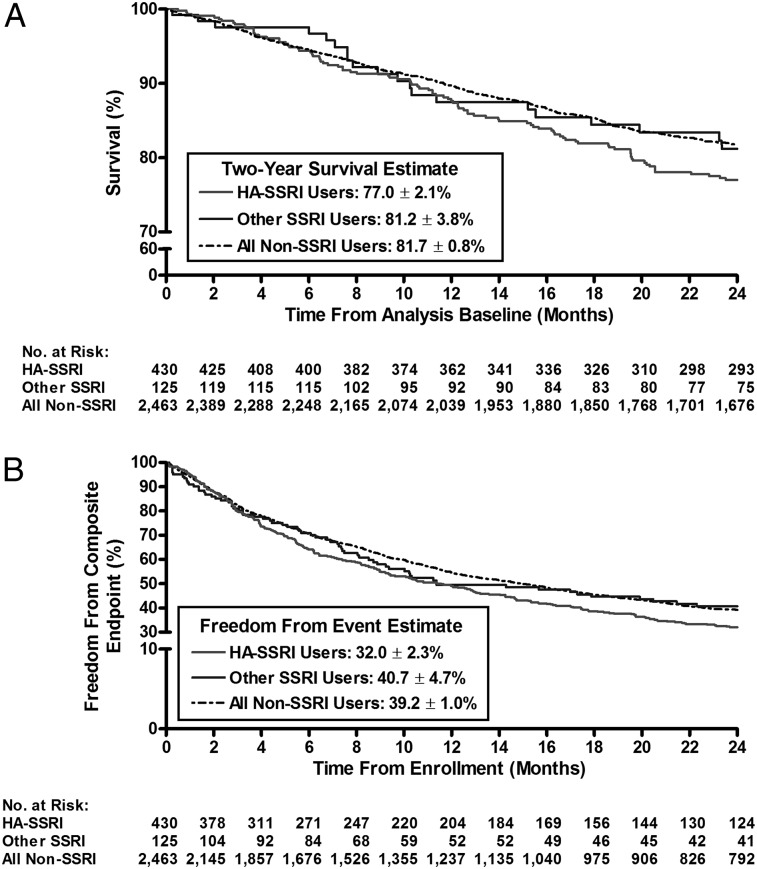
Methods: First, new users (SSRI-naive patients who initiated treatment after enrollment, incident use analysis, n = 220) were matched (1:2) with non-SSRI users (nonusers, n = 440) by enrollment center, sex, date of most recent visit, age, and 6-min walk distance. Second, a cross-sectional design was used to compare nonusers (n = 2,463), high-affinity SSRI users (n = 430), and non-high-affinity SSRI users (n = 125) at enrollment. Mortality and a composite end point defined by events indicative of clinical worsening were evaluated.
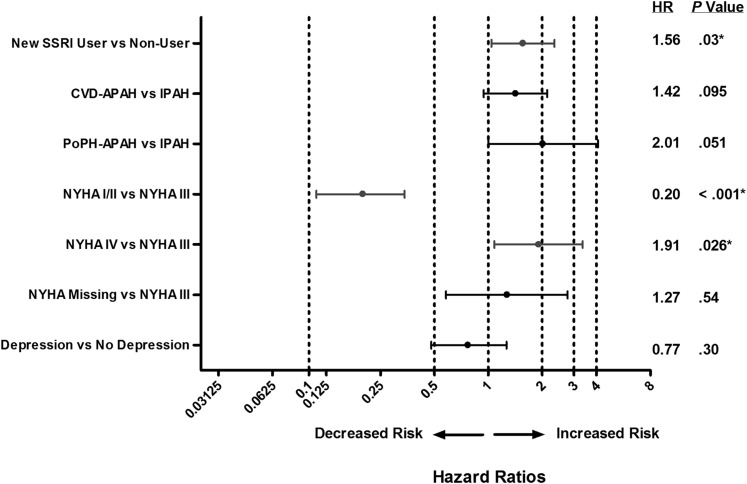
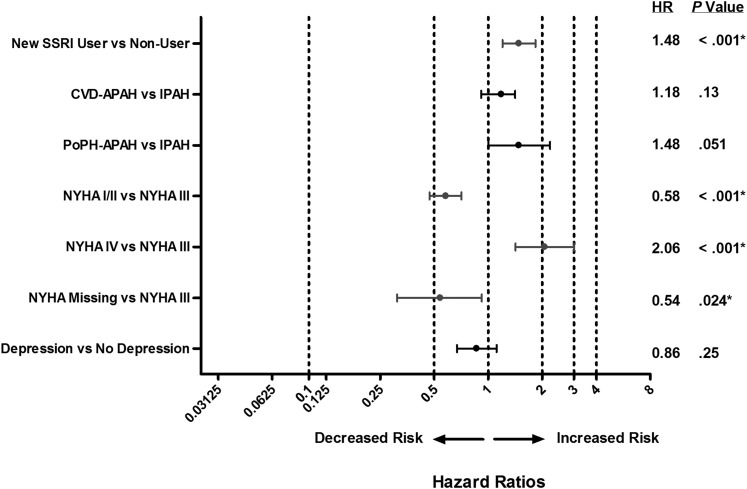
Results: New users had a higher risk of death (unadjusted hazard ratio [HR], 1.74; 95% CI, 1.19-2.54; P = .004) and were less likely to be free from the composite end point 2 years after enrollment vs nonusers (25.7% vs 43.2%, respectively; P < .001). Similarly, among prevalent SSRI users (patients with a history of SSRI use at enrollment), high-affinity SSRI users were less likely to be free from the composite end point vs nonusers (unadjusted HR, 1.20; 95% CI, 1.07-1.36; P = .003). In both analyses, differences in outcome were maintained after adjustment for clinical variables previously associated with PAH outcomes.
Conclusions: In a large population of patients with PAH, incident SSRI use was associated with increased mortality and a greater risk of clinical worsening, although we could not adjust for all potential confounders.
Figures
Similar articles
-
Selective serotonin reuptake inhibitor use and outcomes in pulmonary arterial hypertension.Pulm Pharmacol Ther. 2006;19(5):370-4. doi: 10.1016/j.pupt.2006.01.001. Epub 2006 Feb 17. Pulm Pharmacol Ther. 2006. PMID: 16483811
-
Selective serotonin reuptake inhibitors and the incidence and outcome of pulmonary hypertension.Chest. 2009 Sep;136(3):694-700. doi: 10.1378/chest.08-2823. Epub 2009 Apr 6. Chest. 2009. PMID: 19349384
-
Selective serotonin reuptake inhibitor use and breast cancer survival: a population-based cohort study.Breast Cancer Res. 2018 Jan 19;20(1):4. doi: 10.1186/s13058-017-0928-0. Breast Cancer Res. 2018. PMID: 29351761 Free PMC article.
-
Selective Serotonin Reuptake Inhibitors and Persistent Pulmonary Hypertension of the Newborn: An Update Meta-Analysis.J Womens Health (Larchmt). 2019 Mar;28(3):331-338. doi: 10.1089/jwh.2018.7319. Epub 2018 Nov 8. J Womens Health (Larchmt). 2019. PMID: 30407100 Review.
-
Keep an eye on the SSRI: help avoid possible sight-threatening adverse events.Br J Gen Pract. 2016 Feb;66(643):91. doi: 10.3399/bjgp16X683641. Br J Gen Pract. 2016. PMID: 26823253 Free PMC article. Review. No abstract available.
Cited by
-
Selective Inhibition of Peripheral Serotonin Synthesis in Pulmonary Hypertension.JACC Basic Transl Sci. 2024 Jul 22;9(7):903-905. doi: 10.1016/j.jacbts.2024.05.009. eCollection 2024 Jul. JACC Basic Transl Sci. 2024. PMID: 39170951 Free PMC article.
-
Stimulants and Pulmonary Arterial Hypertension: An Update.Adv Pulm Hypertens. 2018;17(2):49-54. doi: 10.21693/1933-088X-17.2.49. Adv Pulm Hypertens. 2018. PMID: 31656550 Free PMC article.
-
Depression in pulmonary arterial hypertension and interstitial lung diseases.N Am J Med Sci. 2014 Jun;6(6):240-9. doi: 10.4103/1947-2714.134368. N Am J Med Sci. 2014. PMID: 25006558 Free PMC article. Review.
-
Future perspectives in pulmonary arterial hypertension.Eur Respir Rev. 2016 Dec;25(142):381-389. doi: 10.1183/16000617.0084-2016. Eur Respir Rev. 2016. PMID: 27903660 Free PMC article. Review.
-
Hemodynamic effects of fluoxetine in pulmonary arterial hypertension: an open label pilot study.Pulm Circ. 2020 Nov 25;10(4):2045894020971954. doi: 10.1177/2045894020971954. eCollection 2020 Oct-Dec. Pulm Circ. 2020. PMID: 33282204 Free PMC article.
References
-
- Marcos E, Adnot S, Pham MH, et al. Serotonin transporter inhibitors protect against hypoxic pulmonary hypertension. Am J Respir Crit Care Med. 2003;168(4):487-493. - PubMed
-
- Kay JM, Crawford N, Heath D. Blood 5-hydroxytryptamine in rats with pulmonary hypertension produced by ingestion of Crotalaria spectabilis seeds. Experientia. 1968;24(11):1149-1150. - PubMed
-
- Abenhaim L, Moride Y, Brenot F, et al. ; International Primary Pulmonary Hypertension Study Group. Appetite-suppressant drugs and the risk of primary pulmonary hypertension. N Engl J Med. 1996;335(9):609-616. - PubMed
-
- Rothman RB, Ayestas MA, Dersch CM, Baumann MH. Aminorex, fenfluramine, and chlorphentermine are serotonin transporter substrates. Implications for primary pulmonary hypertension. Circulation. 1999;100(8):869-875. - PubMed
-
- Hervé P, Launay JM, Scrobohaci ML, et al. Increased plasma serotonin in primary pulmonary hypertension. Am J Med. 1995;99(3):249-254. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
