

Clinical utility and analytical challenges in measurement of cerebrospinal fluid amyloid-β(1-42) and τ proteins as Alzheimer disease biomarkers
- PMID: 23519967
- PMCID: PMC4159709
- DOI: 10.1373/clinchem.2013.202937
Clinical utility and analytical challenges in measurement of cerebrospinal fluid amyloid-β(1-42) and τ proteins as Alzheimer disease biomarkers
Abstract
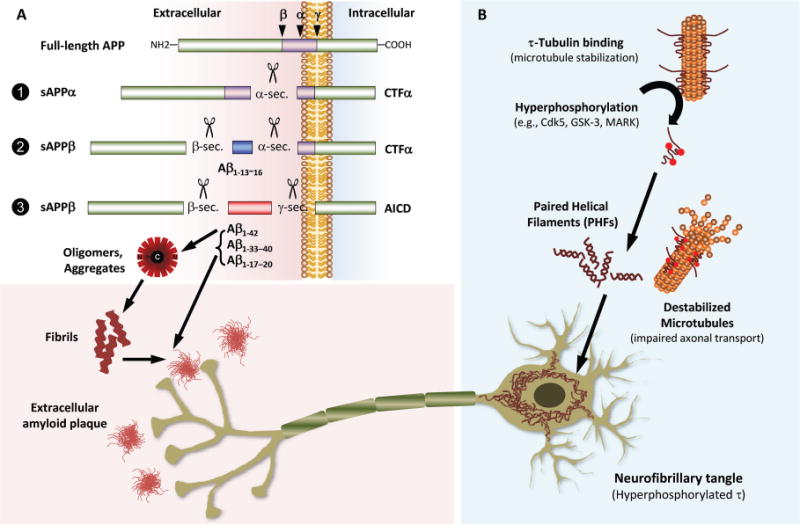
Background: Over the past 2 decades, clinical studies have provided evidence that cerebrospinal fluid (CSF) amyloid β(1-42) (Aβ(1-42)), total τ (t-τ), and τ phosphorylated at Thr181 (p-τ(181)) are reliable biochemical markers of Alzheimer disease (AD) neuropathology.
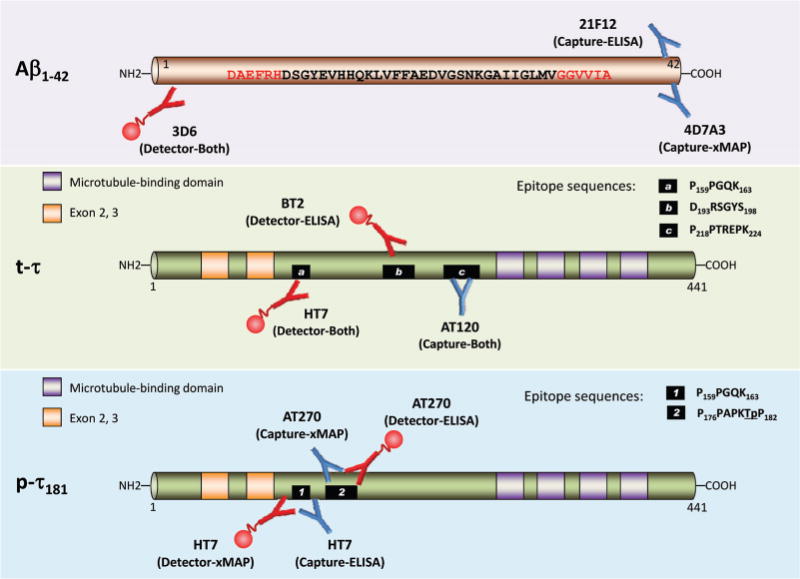
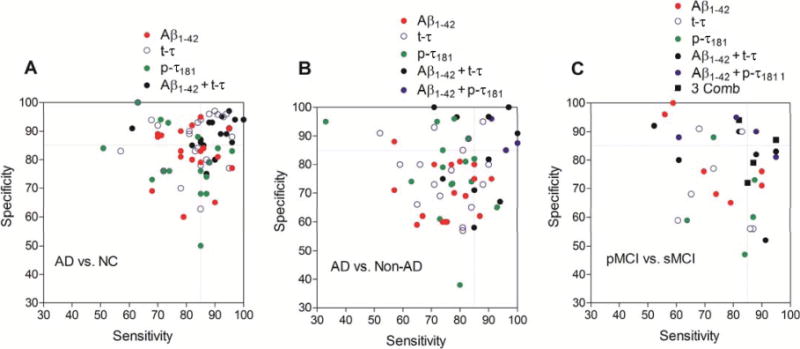
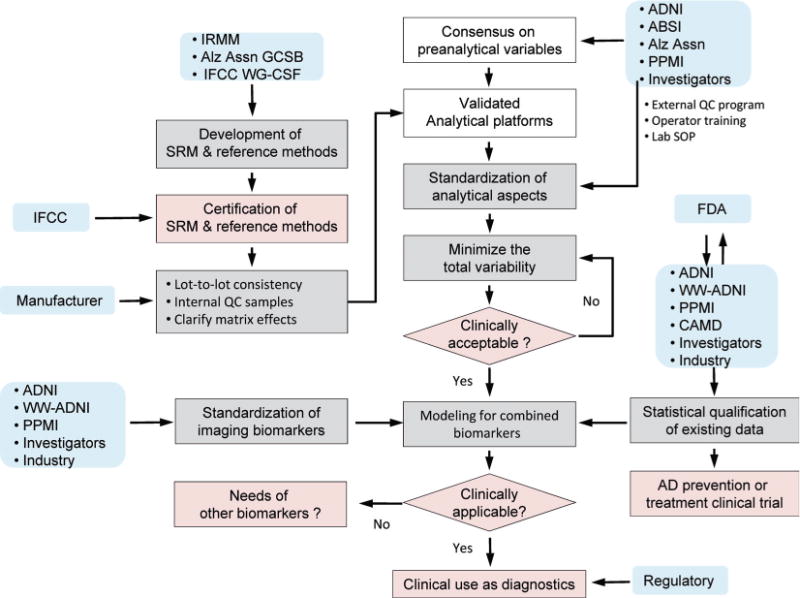
Content: In this review, we summarize the clinical performance and describe the major challenges for the analytical performance of the most widely used immunoassay platforms [based on ELISA or microbead-based multianalyte profiling (xMAP) technology] for the measurement of CSF AD biomarkers (Aβ(1-42), t-τ, and p-τ(181)). With foundational immunoassay data providing the diagnostic and prognostic values of CSF AD biomarkers, the newly revised criteria for the diagnosis of AD include CSF AD biomarkers for use in research settings. In addition, it has been suggested that the selection of AD patients at the predementia stage by use of CSF AD biomarkers can improve the statistical power of clinical trial design. Owing to the lack of a replenishable and commutable human CSF-based standardized reference material (SRM) and significant differences across different immunoassay platforms, the diagnostic-prognostic cutpoints of CSF AD biomarker concentrations are not universal at this time. These challenges can be effectively met in the future, however, through collaborative ongoing standardization efforts to minimize the sources of analytical variability and to develop reference methods and SRMs.
Summary: Measurements of CSF Aβ(1-42), t-τ, and p-τ(181) with analytically qualified immunoassays reliably reflect the neuropathologic hallmarks of AD in patients at the early predementia stage of the disease and even in presymptomatic patients. Thus these CSF biomarker tests are useful for early diagnosis of AD, prediction of disease progression, and efficient design of drug intervention clinical trials.
© 2013 American Association for Clinical Chemistry.
Conflict of interest statement
Figures
Similar articles
-
Simultaneous analysis of cerebrospinal fluid biomarkers using microsphere-based xMAP multiplex technology for early detection of Alzheimer's disease.Methods. 2012 Apr;56(4):484-93. doi: 10.1016/j.ymeth.2012.03.023. Epub 2012 Apr 6. Methods. 2012. PMID: 22503777 Review.
-
Qualification of the analytical and clinical performance of CSF biomarker analyses in ADNI.Acta Neuropathol. 2011 May;121(5):597-609. doi: 10.1007/s00401-011-0808-0. Epub 2011 Feb 11. Acta Neuropathol. 2011. PMID: 21311900 Free PMC article.
-
Decreased beta-amyloid1-42 and increased tau levels in cerebrospinal fluid of patients with Alzheimer disease.JAMA. 2003 Apr 23-30;289(16):2094-103. doi: 10.1001/jama.289.16.2094. JAMA. 2003. PMID: 12709467
-
Simultaneous measurement of beta-amyloid(1-42), total tau, and phosphorylated tau (Thr181) in cerebrospinal fluid by the xMAP technology.Clin Chem. 2005 Feb;51(2):336-45. doi: 10.1373/clinchem.2004.039347. Epub 2004 Nov 24. Clin Chem. 2005. PMID: 15563479 Clinical Trial.
-
Advances in the development of biomarkers for Alzheimer's disease: from CSF total tau and Abeta(1-42) proteins to phosphorylated tau protein.Brain Res Bull. 2003 Aug 15;61(3):243-53. doi: 10.1016/s0361-9230(03)00087-x. Brain Res Bull. 2003. PMID: 12909294 Review.
Cited by
-
Role of cerebrospinal fluid biomarkers in clinical trials for Alzheimer's disease modifying therapies.Korean J Physiol Pharmacol. 2014 Dec;18(6):447-56. doi: 10.4196/kjpp.2014.18.6.447. Epub 2014 Dec 30. Korean J Physiol Pharmacol. 2014. PMID: 25598657 Free PMC article. Review.
-
Harnessing Cerebrospinal Fluid Biomarkers in Clinical Trials for Treating Alzheimer's and Parkinson's Diseases: Potential and Challenges.J Clin Neurol. 2016 Oct;12(4):381-392. doi: 10.3988/jcn.2016.12.4.381. J Clin Neurol. 2016. PMID: 27819412 Free PMC article. Review.
-
Free-water imaging of the hippocampus is a sensitive marker of Alzheimer's disease.Neuroimage Clin. 2019;24:101985. doi: 10.1016/j.nicl.2019.101985. Epub 2019 Aug 22. Neuroimage Clin. 2019. PMID: 31470214 Free PMC article.
-
Detection of early-stage Alzheimer's pathology using blood-based autoantibody biomarkers in elderly hip fracture repair patients.PLoS One. 2019 Nov 15;14(11):e0225178. doi: 10.1371/journal.pone.0225178. eCollection 2019. PLoS One. 2019. PMID: 31730624 Free PMC article.
-
An electrochemiluminescence immunosensor for myoglobin using an indium tin oxide glass electrode modified with gold nanoparticles and platinum nanowires.Mikrochim Acta. 2019 Aug 2;186(9):598. doi: 10.1007/s00604-019-3703-3. Mikrochim Acta. 2019. PMID: 31376022
References
-
- Peskind ER, Riekse R, Quinn JF, Kaye J, Clark CM, Farlow MR, et al. Safety and acceptability of the research lumbar puncture. Alzheimer Dis Assoc Disord. 2005;19:220–5. - PubMed
-
- Dubois B, Feldman HH, Jacova C, DeKosky ST, Barberger-Gateau P, Cummings J, et al. Research criteria for the diagnosis of Alzheimer’s disease: revising the NINCDS-ADRDA criteria. Lancet Neurol. 2007;6:734–46. - PubMed
-
- Hardy J, Selkoe DJ. The amyloid hypothesis of Alzheimer’s disease: progress and problems on the road to therapeutics. Science. 2002;297:353–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
