

Molecular genetics and functional anomalies in a series of 248 Brugada cases with 11 mutations in the TRPM4 channel
- PMID: 23382873
- PMCID: PMC3559649
- DOI: 10.1371/journal.pone.0054131
Molecular genetics and functional anomalies in a series of 248 Brugada cases with 11 mutations in the TRPM4 channel
Abstract
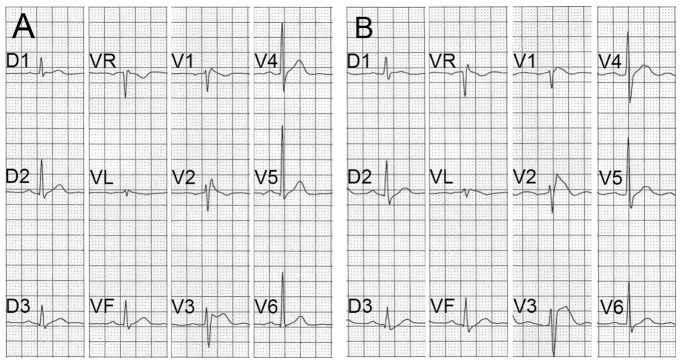
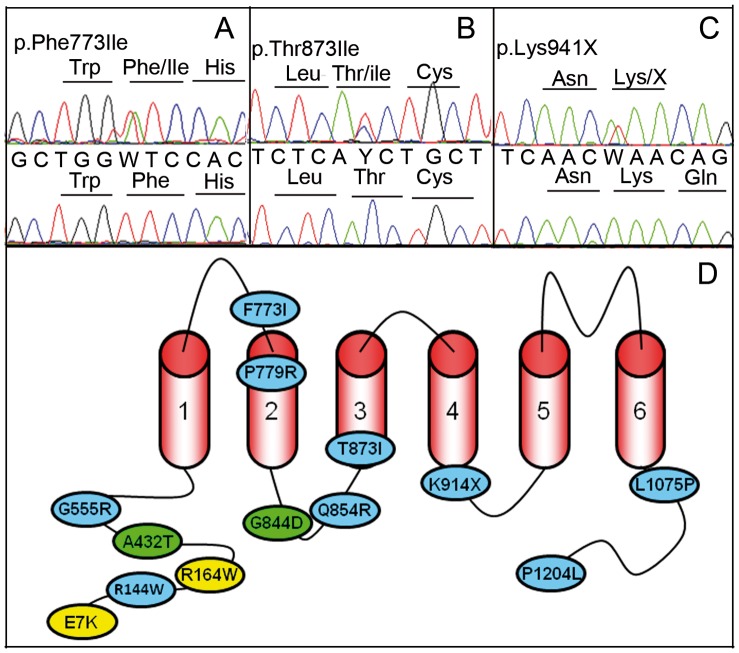
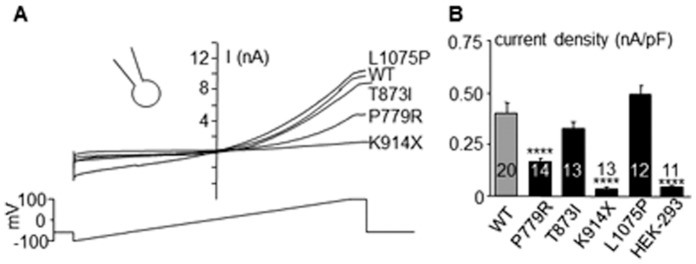
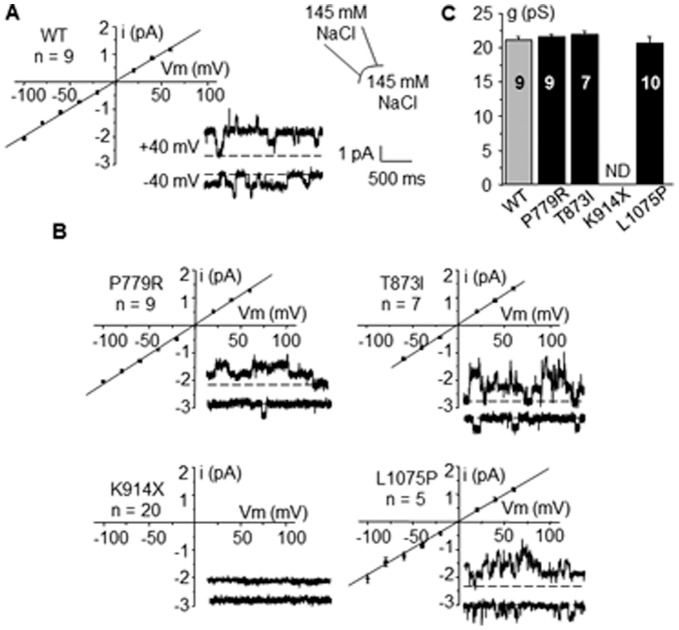
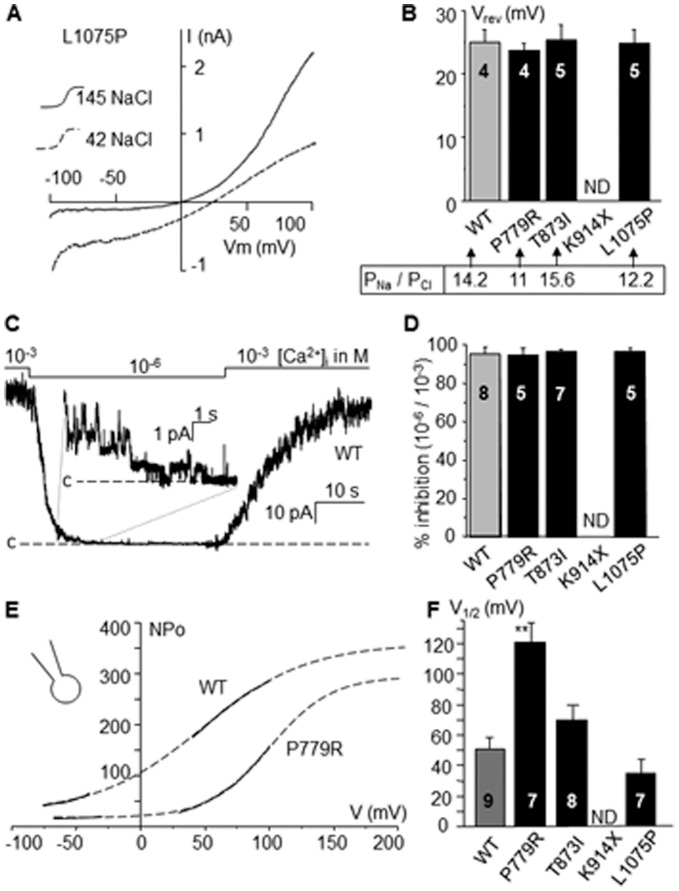
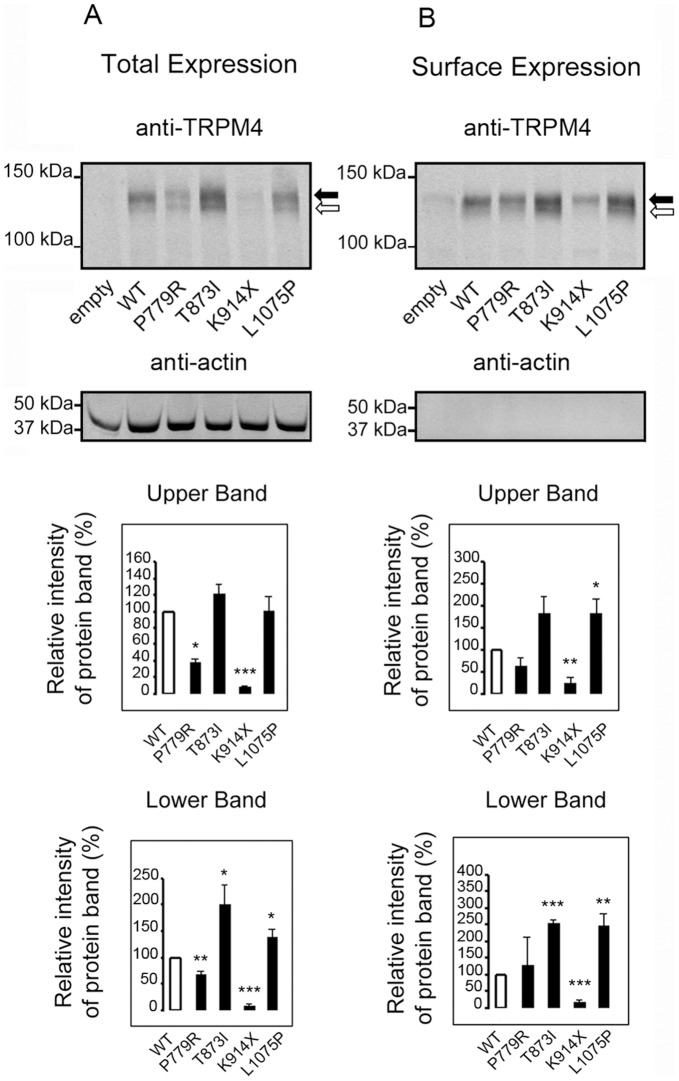
Brugada syndrome (BrS) is a condition defined by ST-segment alteration in right precordial leads and a risk of sudden death. Because BrS is often associated with right bundle branch block and the TRPM4 gene is involved in conduction blocks, we screened TRPM4 for anomalies in BrS cases. The DNA of 248 BrS cases with no SCN5A mutations were screened for TRPM4 mutations. Among this cohort, 20 patients had 11 TRPM4 mutations. Two mutations were previously associated with cardiac conduction blocks and 9 were new mutations (5 absent from ~14'000 control alleles and 4 statistically more prevalent in this BrS cohort than in control alleles). In addition to Brugada, three patients had a bifascicular block and 2 had a complete right bundle branch block. Functional and biochemical studies of 4 selected mutants revealed that these mutations resulted in either a decreased expression (p.Pro779Arg and p.Lys914X) or an increased expression (p.Thr873Ile and p.Leu1075Pro) of TRPM4 channel. TRPM4 mutations account for about 6% of BrS. Consequences of these mutations are diverse on channel electrophysiological and cellular expression. Because of its effect on the resting membrane potential, reduction or increase of TRPM4 channel function may both reduce the availability of sodium channel and thus lead to BrS.
Conflict of interest statement
Figures
Similar articles
-
Single-cell transcriptomics trajectory and molecular convergence of clinically relevant mutations in Brugada syndrome.Am J Physiol Heart Circ Physiol. 2021 May 1;320(5):H1935-H1948. doi: 10.1152/ajpheart.00061.2021. Epub 2021 Apr 2. Am J Physiol Heart Circ Physiol. 2021. PMID: 33797273
-
TRPM4 mutations to cause autosomal recessive and not autosomal dominant Brugada type 1 syndrome.Eur J Med Genet. 2019 Jun;62(6):103527. doi: 10.1016/j.ejmg.2018.08.008. Epub 2018 Aug 22. Eur J Med Genet. 2019. PMID: 30142439
-
Distinct functional defect of three novel Brugada syndrome related cardiac sodium channel mutations.J Biomed Sci. 2009 Feb 20;16(1):23. doi: 10.1186/1423-0127-16-23. J Biomed Sci. 2009. PMID: 19272188 Free PMC article.
-
Brugada syndrome.Orphanet J Rare Dis. 2006 Sep 14;1:35. doi: 10.1186/1750-1172-1-35. Orphanet J Rare Dis. 2006. PMID: 16972995 Free PMC article. Review.
-
TRPM4 channels in the cardiovascular system.Curr Opin Pharmacol. 2014 Apr;15:68-73. doi: 10.1016/j.coph.2013.12.003. Epub 2013 Dec 25. Curr Opin Pharmacol. 2014. PMID: 24721656 Review.
Cited by
-
Variants in the SCN5A Promoter Associated With Various Arrhythmia Phenotypes.J Am Heart Assoc. 2016 Sep 13;5(9):e003644. doi: 10.1161/JAHA.116.003644. J Am Heart Assoc. 2016. PMID: 27625342 Free PMC article.
-
Deletion of Trpm4 Alters the Function of the Nav1.5 Channel in Murine Cardiac Myocytes.Int J Mol Sci. 2021 Mar 26;22(7):3401. doi: 10.3390/ijms22073401. Int J Mol Sci. 2021. PMID: 33810249 Free PMC article.
-
The Brugada Syndrome: A Rare Arrhythmia Disorder with Complex Inheritance.Front Cardiovasc Med. 2016 Apr 25;3:9. doi: 10.3389/fcvm.2016.00009. eCollection 2016. Front Cardiovasc Med. 2016. PMID: 27200363 Free PMC article. Review.
-
Pharmacological Modulation and (Patho)Physiological Roles of TRPM4 Channel-Part 2: TRPM4 in Health and Disease.Pharmaceuticals (Basel). 2021 Dec 28;15(1):40. doi: 10.3390/ph15010040. Pharmaceuticals (Basel). 2021. PMID: 35056097 Free PMC article. Review.
-
Store-Operated Ca2+ Entry as a Prostate Cancer Biomarker - a Riddle with Perspectives.Curr Mol Biol Rep. 2017;3(4):208-217. doi: 10.1007/s40610-017-0072-8. Epub 2017 Oct 28. Curr Mol Biol Rep. 2017. PMID: 29951353 Free PMC article. Review.
References
-
- Brugada P, Brugada J (1992) Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol 20: 1391–1396. - PubMed
-
- Brugada J, Brugada R, Antzelevitch C, Towbin J, Nademanee K, et al. (2002) Long-term follow-up of individuals with the electrocardiographic pattern of right bundle-branch block and ST-segment elevation in precordial leads V1 to V3. Circulation 105: 73–78. - PubMed
-
- Priori SG, Napolitano C, Gasparini M, Pappone C, Della Bella P, et al. (2002) Natural history of Brugada syndrome: insights for risk stratification and management. Circulation 105: 1342–1347. - PubMed
-
- Shimizu W, Antzelevitch C, Suyama K, Kurita T, Taguchi A, et al. (2000) Effect of sodium channel blockers on ST segment, QRS duration, and corrected QT interval in patients with Brugada syndrome. J Cardiovasc Electrophysiol 11: 1320–1329. - PubMed
-
- Antzelevitch C, Brugada P, Borggrefe M, Brugada J, Brugada R, et al. (2005) Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation 111: 659–670. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
