

Effects of folic acid supplementation on overall and site-specific cancer incidence during the randomised trials: meta-analyses of data on 50,000 individuals
- PMID: 23352552
- PMCID: PMC3836669
- DOI: 10.1016/S0140-6736(12)62001-7
Effects of folic acid supplementation on overall and site-specific cancer incidence during the randomised trials: meta-analyses of data on 50,000 individuals
Abstract
Background: Some countries fortify flour with folic acid to prevent neural tube defects but others do not, partly because of concerns about possible cancer risks. We aimed to assess any effects on site-specific cancer rates in the randomised trials of folic acid supplementation, at doses higher than those from fortification.
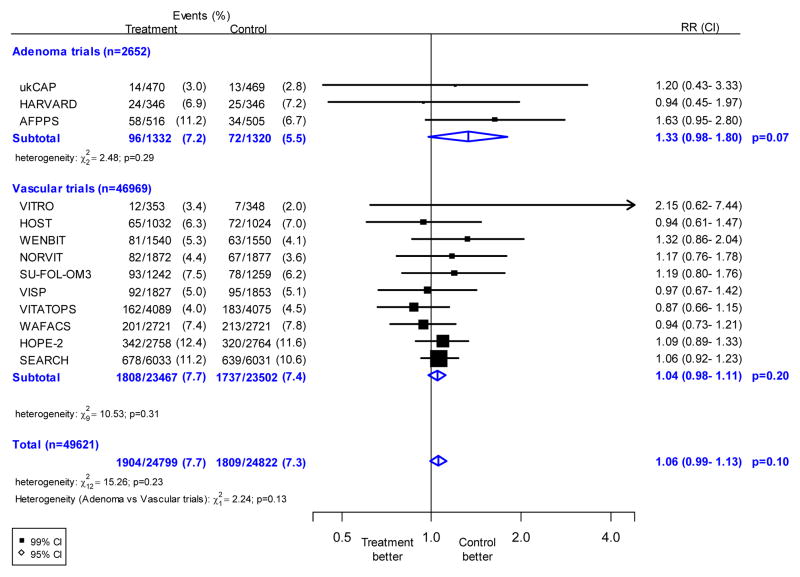
Methods: In these meta-analyses, we sought all trials completed before 2011 that compared folic acid versus placebo, had scheduled treatment duration at least 1 year, included at least 500 participants, and recorded data on cancer incidence. We obtained individual participant datasets that included 49,621 participants in all 13 such trials (ten trials of folic acid for prevention of cardiovascular disease [n=46,969] and three trials in patients with colorectal adenoma [n=2652]). All these trials were evenly randomised. The main outcome was incident cancer (ignoring non-melanoma skin cancer) during the scheduled treatment period (among participants who were still free of cancer). We compared those allocated folic acid with those allocated placebo, and used log-rank analyses to calculate the cancer incidence rate ratio (RR).
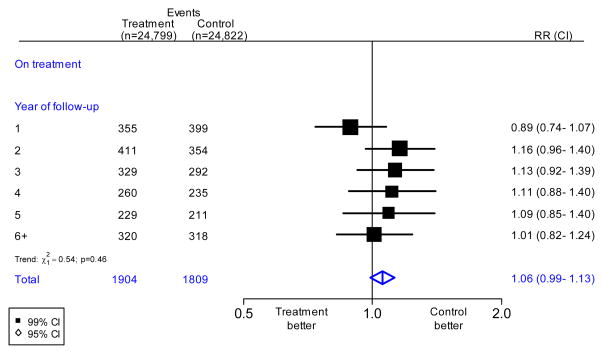
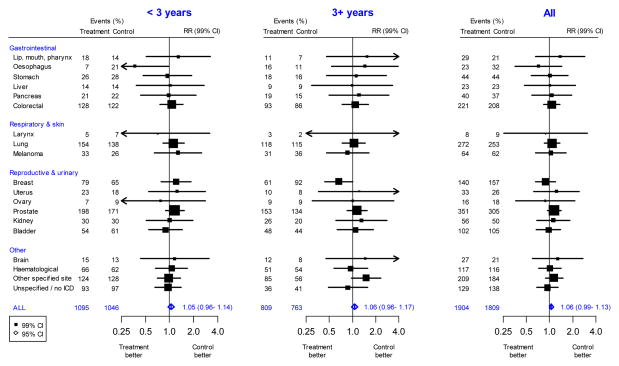
Findings: During a weighted average scheduled treatment duration of 5·2 years, allocation to folic acid quadrupled plasma concentrations of folic acid (57·3 nmol/L for the folic acid groups vs 13·5 nmol/L for the placebo groups), but had no significant effect on overall cancer incidence (1904 cancers in the folic acid groups vs 1809 cancers in the placebo groups, RR 1·06, 95% CI 0·99–1·13, p=0·10). There was no trend towards greater effect with longer treatment. There was no significant heterogeneity between the results of the 13 individual trials (p=0·23), or between the two overall results in the cadiovascular prevention trials and the adenoma trials (p=0·13). Moreover, there was no significant effect of folic acid supplementation on the incidence of cancer of the large intestine, prostate, lung, breast, or any other specific site.
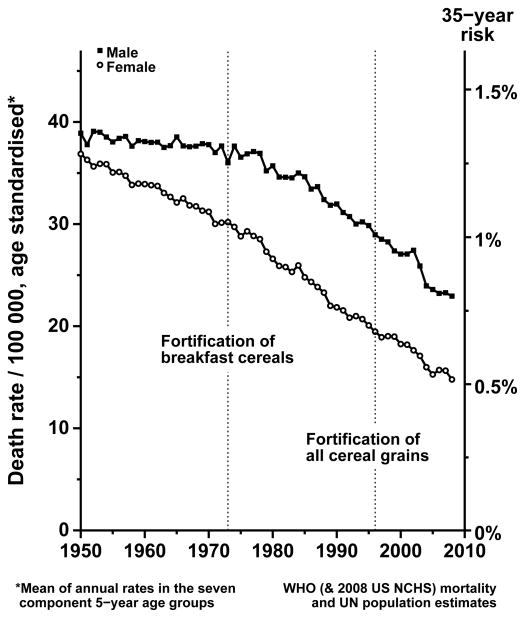
Interpretation: Folic acid supplementation does not substantially increase or decrease incidence of site-specific cancer during the first 5 years of treatment. Fortification of flour and other cereal products involves doses of folic acid that are, on average, an order of magnitude smaller than the doses used in these trials.
Funding: British Heart Foundation, Medical Research Council, Cancer Research UK, Food Standards Agency.
Conflict of interest statement
Figures
Comment in
-
Folic acid and cancer--where are we today?Lancet. 2013 Mar 23;381(9871):974-6. doi: 10.1016/S0140-6736(13)60110-5. Lancet. 2013. PMID: 23352551 No abstract available.
Similar articles
-
Folic acid supplementation and cancer risk: a meta-analysis of randomized controlled trials.Int J Cancer. 2013 Sep 1;133(5):1033-41. doi: 10.1002/ijc.28038. Epub 2013 Feb 15. Int J Cancer. 2013. PMID: 23338728 Review.
-
Folic acid for the prevention of colorectal adenomas: a randomized clinical trial.JAMA. 2007 Jun 6;297(21):2351-9. doi: 10.1001/jama.297.21.2351. JAMA. 2007. PMID: 17551129 Clinical Trial.
-
Folic Acid and Vitamin B12 Supplementation and the Risk of Cancer: Long-term Follow-up of the B Vitamins for the Prevention of Osteoporotic Fractures (B-PROOF) Trial.Cancer Epidemiol Biomarkers Prev. 2019 Feb;28(2):275-282. doi: 10.1158/1055-9965.EPI-17-1198. Epub 2018 Oct 19. Cancer Epidemiol Biomarkers Prev. 2019. PMID: 30341095 Clinical Trial.
-
Meta-analysis of cancer risk in folic acid supplementation trials.Cancer Epidemiol. 2012 Feb;36(1):78-81. doi: 10.1016/j.canep.2011.05.003. Epub 2011 Oct 21. Cancer Epidemiol. 2012. PMID: 22018948
-
Folic acid to reduce neonatal mortality from neural tube disorders.Int J Epidemiol. 2010 Apr;39 Suppl 1(Suppl 1):i110-21. doi: 10.1093/ije/dyq028. Int J Epidemiol. 2010. PMID: 20348114 Free PMC article. Review.
Cited by
-
Epidemiology, prenatal management, and prevention of neural tube defects.Saudi Med J. 2014 Dec;35 Suppl 1(Suppl 1):S15-28. Saudi Med J. 2014. PMID: 25551106 Free PMC article. Review.
-
Folic acid in pregnancy and mortality from cancer and cardiovascular disease: further follow-up of the Aberdeen folic acid supplementation trial.J Epidemiol Community Health. 2015 Aug;69(8):789-94. doi: 10.1136/jech-2014-205324. Epub 2015 Apr 8. J Epidemiol Community Health. 2015. PMID: 25855124 Free PMC article.
-
Simplifying the B Complex: How Vitamins B6 and B9 Modulate One Carbon Metabolism in Cancer and Beyond.Metabolites. 2022 Oct 11;12(10):961. doi: 10.3390/metabo12100961. Metabolites. 2022. PMID: 36295863 Free PMC article. Review.
-
Association Between Folate and Health Outcomes: An Umbrella Review of Meta-Analyses.Front Public Health. 2020 Dec 15;8:550753. doi: 10.3389/fpubh.2020.550753. eCollection 2020. Front Public Health. 2020. PMID: 33384976 Free PMC article.
-
Physical activity, sedentary behaviour, diet, and cancer: an update and emerging new evidence.Lancet Oncol. 2017 Aug;18(8):e457-e471. doi: 10.1016/S1470-2045(17)30411-4. Epub 2017 Jul 26. Lancet Oncol. 2017. PMID: 28759385 Free PMC article. Review.
References
-
- Hibbard BM. The role of folic acid in pregnancy with particular reference to anaemia, abruption and abortion. J Obstet Gynaecol Br Common W. 1964;71:529–42. - PubMed
-
- Bower C, Stanley FJ. Dietary folate as a risk factor for neural tube defects: evidence from a case-control study in Western Australia. Med J Aust. 1989;150:613–19. - PubMed
-
- Smithells RW, Sheppard S, Schorah CJ, et al. Possible prevention of neural tube defects by periconceptional vitamin supplementation. Lancet. 1980;1:339–40. - PubMed
-
- Berry RJ, Li Z, Erickson JD, Li S, Moore CA, Wang H, Mulinare J, Zha P, Wong LY, Gindler J, Hong SX, Correa A. Prevention of neural-tube defects with folic acid in China. China-U.S. Collaborative Project for Neural Tube Defect Prevention. N Engl J Med. 1999;341:1485–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
