

Lifetime risk and age at diagnosis of symptomatic knee osteoarthritis in the US
- PMID: 23203864
- PMCID: PMC3886119
- DOI: 10.1002/acr.21898
Lifetime risk and age at diagnosis of symptomatic knee osteoarthritis in the US
Abstract
Objective: To estimate the incidence and lifetime risk of diagnosed symptomatic knee osteoarthritis (OA) and the age at diagnosis of knee OA based on self-reports in the US population.
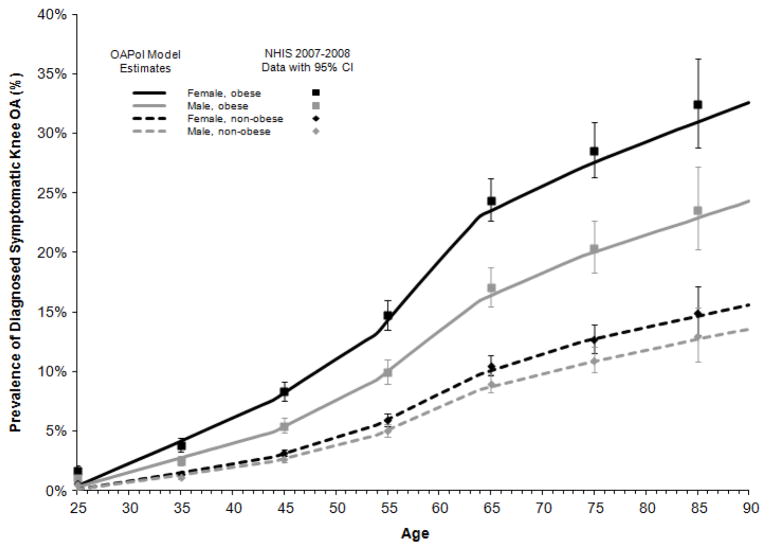
Methods: We estimated the incidence of diagnosed symptomatic knee OA in the US by combining data on age-, sex-, and obesity-specific prevalence from the 2007-2008 National Health Interview Survey, with disease duration estimates derived from the Osteoarthritis Policy (OAPol) Model, a validated computer simulation model of knee OA. We used the OAPol Model to estimate the mean and median ages at diagnosis and lifetime risk.
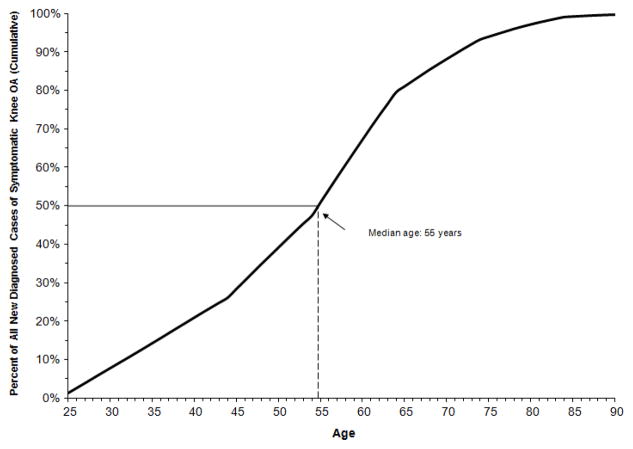
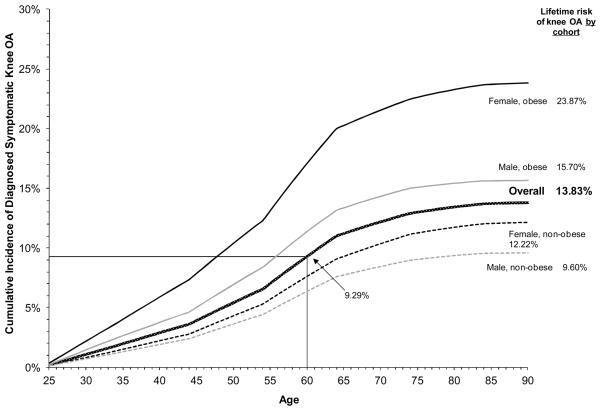
Results: The estimated incidence of diagnosed symptomatic knee OA was highest among adults ages 55-64 years, ranging from 0.37% per year for nonobese men to 1.02% per year for obese women. The estimated median age at knee OA diagnosis was 55 years. The estimated lifetime risk was 13.83%, ranging from 9.60% for nonobese men to 23.87% in obese women. Approximately 9.29% of the US population is diagnosed with symptomatic knee OA by age 60 years.
Conclusion: The diagnosis of symptomatic knee OA occurs relatively early in life, suggesting that prevention programs should be offered relatively early in the life course. Further research is needed to understand the future burden of health care utilization resulting from earlier diagnosis of knee OA.
Copyright © 2013 by the American College of Rheumatology.
Figures
Similar articles
-
Number of Persons With Symptomatic Knee Osteoarthritis in the US: Impact of Race and Ethnicity, Age, Sex, and Obesity.Arthritis Care Res (Hoboken). 2016 Dec;68(12):1743-1750. doi: 10.1002/acr.22897. Epub 2016 Nov 3. Arthritis Care Res (Hoboken). 2016. PMID: 27014966 Free PMC article.
-
Forecasting the burden of advanced knee osteoarthritis over a 10-year period in a cohort of 60-64 year-old US adults.Osteoarthritis Cartilage. 2011 Jan;19(1):44-50. doi: 10.1016/j.joca.2010.10.009. Epub 2010 Oct 16. Osteoarthritis Cartilage. 2011. PMID: 20955807 Free PMC article.
-
Annual Incidence of Knee Symptoms and Four Knee Osteoarthritis Outcomes in the Johnston County Osteoarthritis Project.Arthritis Care Res (Hoboken). 2016 Jan;68(1):55-65. doi: 10.1002/acr.22641. Arthritis Care Res (Hoboken). 2016. PMID: 26097226 Free PMC article.
-
The effect of osteoarthritis definition on prevalence and incidence estimates: a systematic review.Osteoarthritis Cartilage. 2011 Nov;19(11):1270-85. doi: 10.1016/j.joca.2011.08.009. Epub 2011 Aug 24. Osteoarthritis Cartilage. 2011. PMID: 21907813 Review.
-
[Impact of the distinct diagnostic criteria used in population-based studies on estimation of the prevalence of knee osteoarthritis].Gac Sanit. 2010 Jan-Feb;24(1):28-32. doi: 10.1016/j.gaceta.2009.06.002. Epub 2009 Sep 11. Gac Sanit. 2010. PMID: 19748161 Review. Spanish.
Cited by
-
Exploring Platelet-Rich Plasma Therapy for Knee Osteoarthritis: An In-Depth Analysis.J Funct Biomater. 2024 Aug 9;15(8):221. doi: 10.3390/jfb15080221. J Funct Biomater. 2024. PMID: 39194659 Free PMC article. Review.
-
Transcriptomic changes during the replicative senescence of human articular chondrocytes.bioRxiv [Preprint]. 2023 Nov 7:2023.11.07.565835. doi: 10.1101/2023.11.07.565835. bioRxiv. 2023. Update in: Int J Mol Sci. 2024 Nov 12;25(22):12130. doi: 10.3390/ijms252212130. PMID: 37986862 Free PMC article. Updated. Preprint.
-
Effects of Running in Minimal and Conventional Footwear on Medial Tibiofemoral Cartilage Failure Probability in Habitual and Non-Habitual Users.J Clin Med. 2022 Dec 9;11(24):7335. doi: 10.3390/jcm11247335. J Clin Med. 2022. PMID: 36555951 Free PMC article.
-
A literature review on plant-based foods and dietary quality in knee osteoarthritis.Eur J Rheumatol. 2022 May 10;11(Suppl 1):S32-40. doi: 10.5152/eurjrheum.2022.21134. Online ahead of print. Eur J Rheumatol. 2022. PMID: 35535585 Free PMC article.
-
Efficacy of bisphosphonates in specific knee osteoarthritis subpopulations: protocol for an OA Trial Bank systematic review and individual patient data meta-analysis.BMJ Open. 2018 Dec 19;8(12):e023889. doi: 10.1136/bmjopen-2018-023889. BMJ Open. 2018. PMID: 30573485 Free PMC article.
References
-
- Hochberg MC. Proposed 2011 American College of Rheumatology recommendations for the use of non-pharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip and knee. Paper presented at: Seminars in Arthritis and Rheumatism; 2011. - PubMed
-
- Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis. Part II. Osteoarthritis of the knee. American College of Rheumatology. Arthritis Rheum. 1995 Nov;38(11):1541–1546. - PubMed
-
- Richmond J, Hunter D, Irrgang J, et al. American academy of orthopaedic surgeons clinical practice guideline on the treatment of osteoarthritis (OA) of the knee. J Bone Joint Surg Am. 2010 Apr;92(4):990–993. - PubMed
-
- Zhang W, Nuki G, Moskowitz RW, et al. OARSI recommendations for the management of hip and knee osteoarthritis: Part III: changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis Cartilage. 2010 Apr;18(4):476–499. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
