

Obatoclax, saliphenylhalamide, and gemcitabine inhibit influenza a virus infection
- PMID: 22910914
- PMCID: PMC3471742
- DOI: 10.1074/jbc.M112.392142
Obatoclax, saliphenylhalamide, and gemcitabine inhibit influenza a virus infection
Abstract
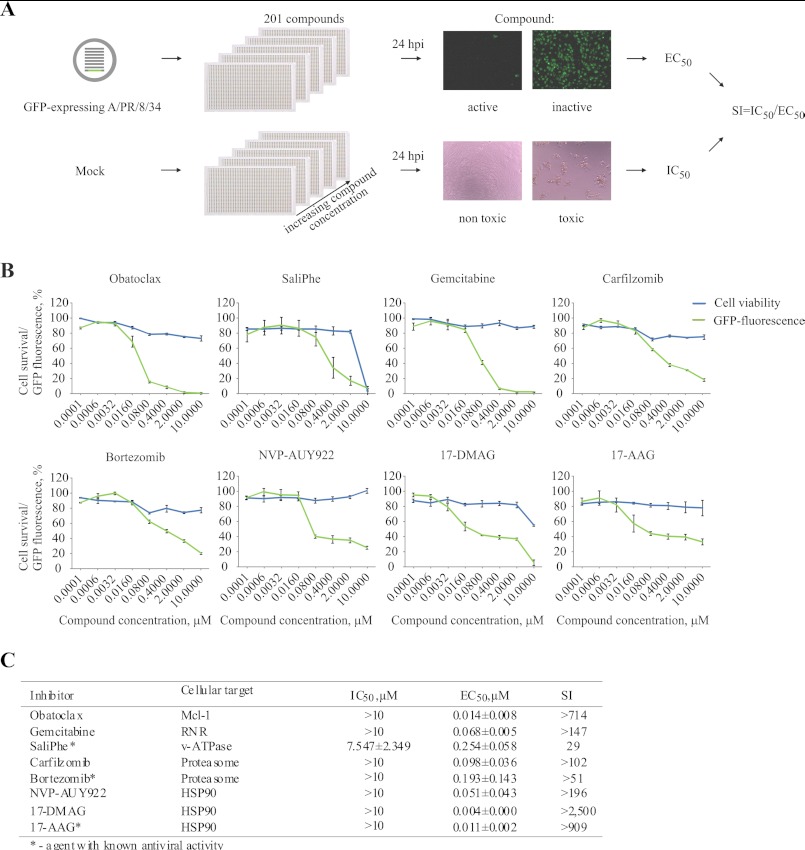
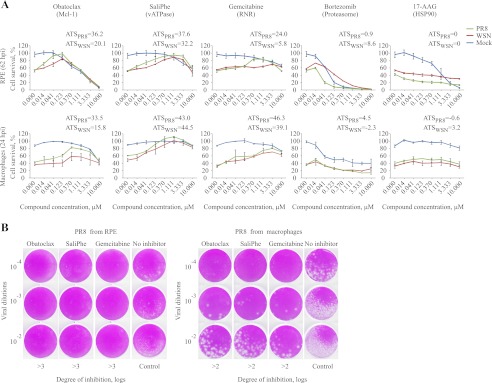
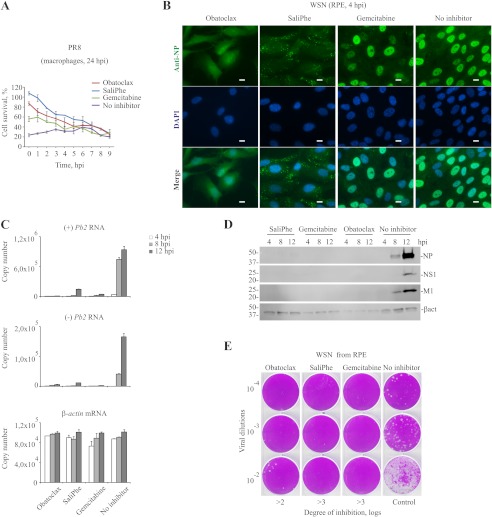
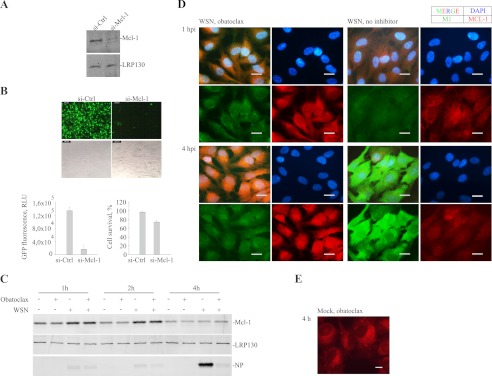
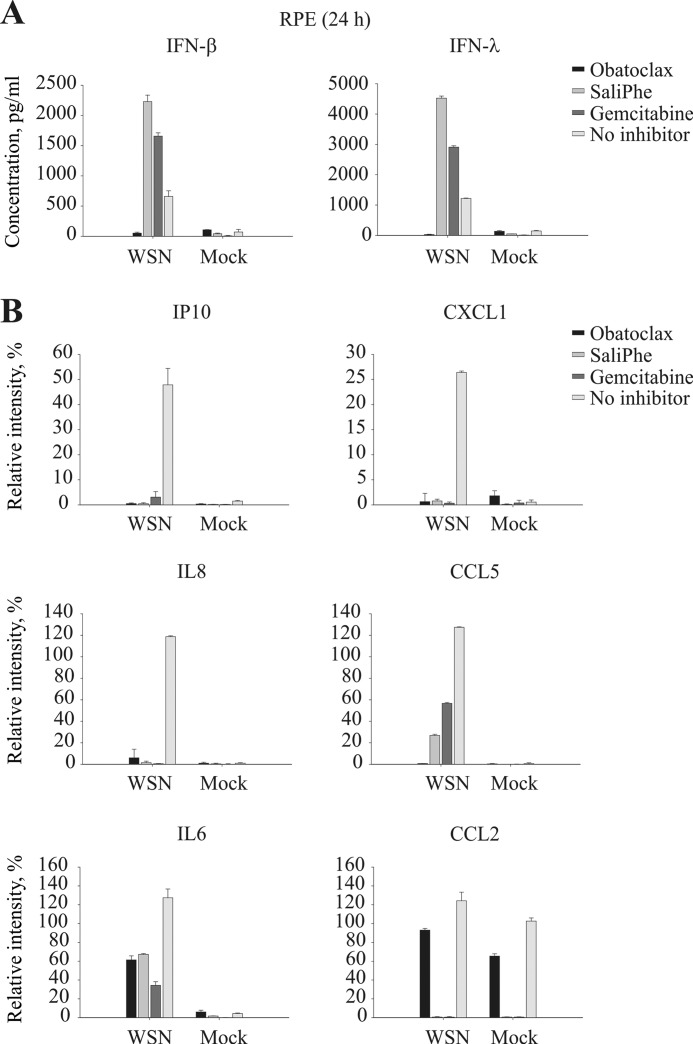
Influenza A viruses (IAVs) infect humans and cause significant morbidity and mortality. Different treatment options have been developed; however, these were insufficient during recent IAV outbreaks. Here, we conducted a targeted chemical screen in human nonmalignant cells to validate known and search for novel host-directed antivirals. The screen validated saliphenylhalamide (SaliPhe) and identified two novel anti-IAV agents, obatoclax and gemcitabine. Further experiments demonstrated that Mcl-1 (target of obatoclax) provides a novel host target for IAV treatment. Moreover, we showed that obatoclax and SaliPhe inhibited IAV uptake and gemcitabine suppressed viral RNA transcription and replication. These compounds possess broad spectrum antiviral activity, although their antiviral efficacies were virus-, cell type-, and species-specific. Altogether, our results suggest that phase II obatoclax, investigational SaliPhe, and FDA/EMEA-approved gemcitabine represent potent antiviral agents.
Figures
Similar articles
-
Immuno-modulating properties of saliphenylhalamide, SNS-032, obatoclax, and gemcitabine.Antiviral Res. 2016 Feb;126:69-80. doi: 10.1016/j.antiviral.2015.12.011. Epub 2015 Dec 29. Antiviral Res. 2016. PMID: 26738783
-
Obatoclax, saliphenylhalamide and gemcitabine inhibit Zika virus infection in vitro and differentially affect cellular signaling, transcription and metabolism.Antiviral Res. 2017 Mar;139:117-128. doi: 10.1016/j.antiviral.2016.12.022. Epub 2016 Dec 31. Antiviral Res. 2017. PMID: 28049006
-
Identification and Characterization of Novel Compounds with Broad-Spectrum Antiviral Activity against Influenza A and B Viruses.J Virol. 2020 Mar 17;94(7):e02149-19. doi: 10.1128/JVI.02149-19. Print 2020 Mar 17. J Virol. 2020. PMID: 31941776 Free PMC article.
-
Inhibition of influenza A virus infection in vitro by saliphenylhalamide-loaded porous silicon nanoparticles.ACS Nano. 2013 Aug 27;7(8):6884-93. doi: 10.1021/nn402062f. Epub 2013 Aug 1. ACS Nano. 2013. PMID: 23889734
-
Berberine and Obatoclax Inhibit SARS-Cov-2 Replication in Primary Human Nasal Epithelial Cells In Vitro.Viruses. 2021 Feb 11;13(2):282. doi: 10.3390/v13020282. Viruses. 2021. PMID: 33670363 Free PMC article.
Cited by
-
Potential Antiviral Options against SARS-CoV-2 Infection.Viruses. 2020 Jun 13;12(6):642. doi: 10.3390/v12060642. Viruses. 2020. PMID: 32545799 Free PMC article.
-
Identification of anisomycin, prodigiosin and obatoclax as compounds with broad-spectrum anti-parasitic activity.PLoS Negl Trop Dis. 2020 Mar 20;14(3):e0008150. doi: 10.1371/journal.pntd.0008150. eCollection 2020 Mar. PLoS Negl Trop Dis. 2020. PMID: 32196500 Free PMC article.
-
Replication-Competent Influenza Virus and Respiratory Syncytial Virus Luciferase Reporter Strains Engineered for Co-Infections Identify Antiviral Compounds in Combination Screens.Biochemistry. 2015 Sep 15;54(36):5589-604. doi: 10.1021/acs.biochem.5b00623. Epub 2015 Sep 1. Biochemistry. 2015. PMID: 26307636 Free PMC article.
-
Drug Repurposing Approaches for the Treatment of Influenza Viral Infection: Reviving Old Drugs to Fight Against a Long-Lived Enemy.Front Immunol. 2019 Mar 19;10:531. doi: 10.3389/fimmu.2019.00531. eCollection 2019. Front Immunol. 2019. PMID: 30941148 Free PMC article. Review.
-
Antiviral Properties of Chemical Inhibitors of Cellular Anti-Apoptotic Bcl-2 Proteins.Viruses. 2017 Sep 25;9(10):271. doi: 10.3390/v9100271. Viruses. 2017. PMID: 28946654 Free PMC article.
References
-
- Kurtz J., Manvell R. J., Banks J. (1996) Avian influenza virus isolated from a woman with conjunctivitis. Lancet 348, 901–902 - PubMed
-
- Müller K. H., Kakkola L., Nagaraj A. S., Cheltsov A. V., Anastasina M., Kainov D. E. (2012) Emerging cellular targets for influenza antiviral agents. Trends Pharm. Sci. 33, 89–99 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
