

Frontotemporal dementia due to C9ORF72 mutations: clinical and imaging features
- PMID: 22875087
- PMCID: PMC3430713
- DOI: 10.1212/WNL.0b013e318268452e
Frontotemporal dementia due to C9ORF72 mutations: clinical and imaging features
Abstract
Objective: To describe the phenotype of patients with C9FTD/ALS (C9ORF72) hexanucleotide repeat expansion.
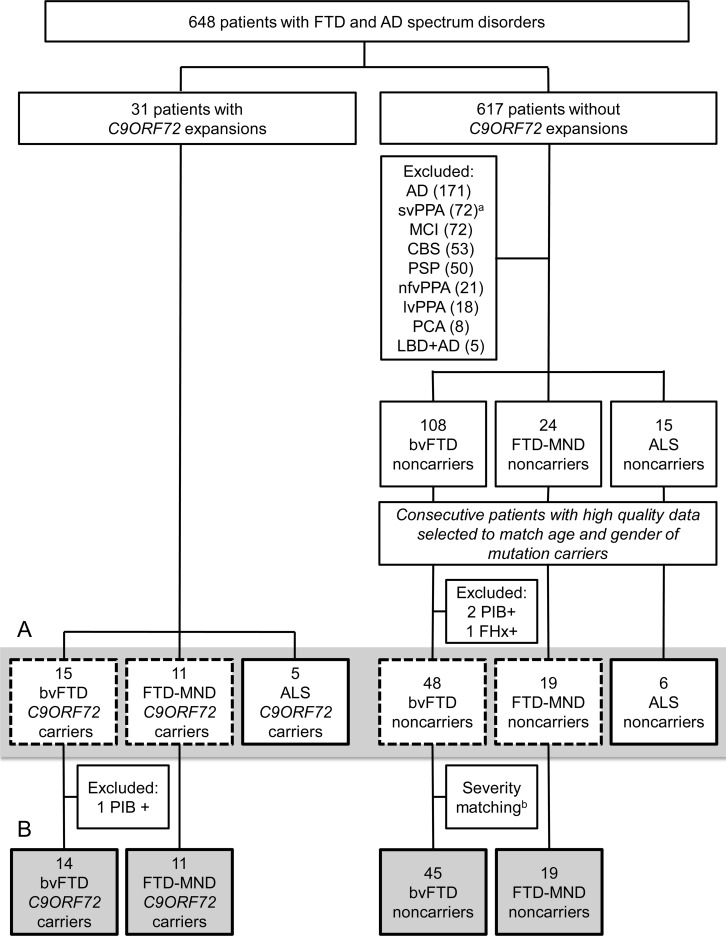
Methods: A total of 648 patients with frontotemporal dementia (FTD)-related clinical diagnoses and Alzheimer disease (AD) dementia were tested for C9ORF72 expansion and 31 carried expanded repeats (C9+). Clinical and neuroimaging data were compared between C9+ (15 behavioral variant FTD [bvFTD], 11 FTD-motor neuron disease [MND], 5 amyotrophic lateral sclerosis [ALS]) and sporadic noncarriers (48 bvFTD, 19 FTD-MND, 6 ALS).
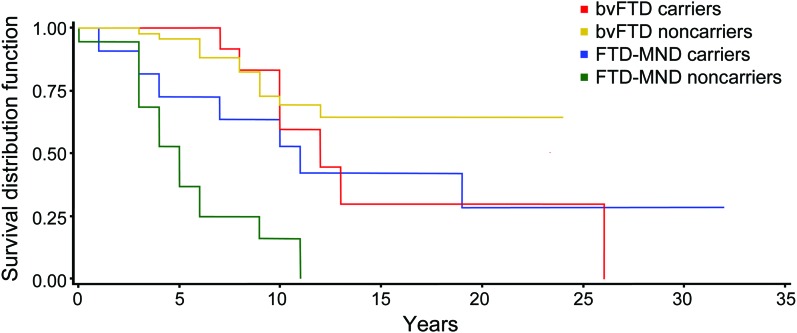
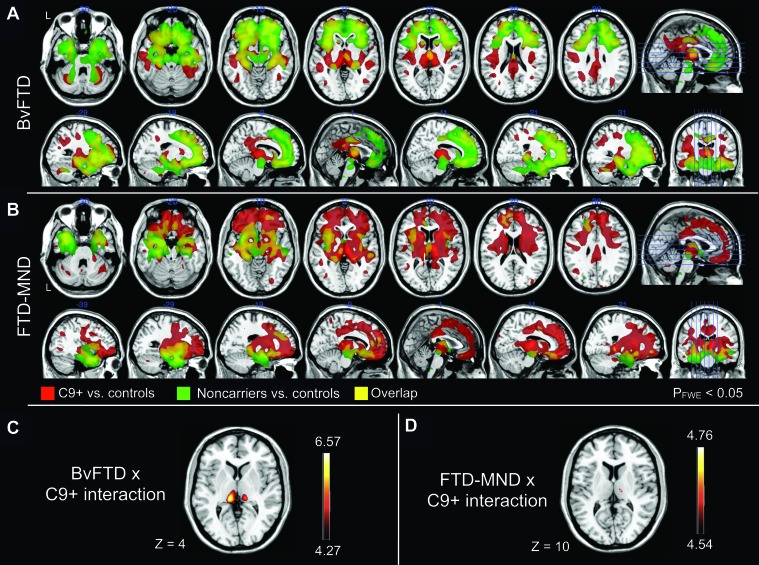
Results: All C9+ patients displayed clinical syndromes of bvFTD, ALS, or FTD-MND. At first evaluation, C9+ bvFTD patients had more delusions and greater impairment of working memory, but milder eating dysregulation compared to bvFTD noncarriers. C9+FTD-MND patients had a trend for longer survival and had an earlier age at onset than FTD-MND noncarriers. Voxel-based morphometry demonstrated more thalamic atrophy in FTD and FTD-MND carriers than in noncarriers.
Conclusions: Patients with the C9ORF72 hexanucleotide repeat expansion develop bvFTD, ALS, or FTD-MND with similar clinical and imaging features to sporadic cases. Other FTD spectrum diagnoses and AD dementia appear rare or absent among C9+ individuals. Longer survival in C9+ FTD-MND suggests slower disease progression and thalamic atrophy represents a novel and unexpected feature.
Figures
Comment in
-
FTD/ALS families are no longer orphaned: the C9ORF72 story.Neurology. 2012 Sep 4;79(10):962-4. doi: 10.1212/WNL.0b013e318268471a. Epub 2012 Aug 8. Neurology. 2012. PMID: 22875094 No abstract available.
Similar articles
-
Longitudinal imaging in C9orf72 mutation carriers: Relationship to phenotype.Neuroimage Clin. 2016 Oct 22;12:1035-1043. doi: 10.1016/j.nicl.2016.10.014. eCollection 2016. Neuroimage Clin. 2016. PMID: 27995069 Free PMC article. Clinical Trial.
-
Clinical and neuropathologic heterogeneity of c9FTD/ALS associated with hexanucleotide repeat expansion in C9ORF72.Acta Neuropathol. 2011 Dec;122(6):673-90. doi: 10.1007/s00401-011-0907-y. Epub 2011 Nov 15. Acta Neuropathol. 2011. PMID: 22083254 Free PMC article.
-
Atypical, slowly progressive behavioural variant frontotemporal dementia associated with C9ORF72 hexanucleotide expansion.J Neurol Neurosurg Psychiatry. 2012 Apr;83(4):358-64. doi: 10.1136/jnnp-2011-301883. J Neurol Neurosurg Psychiatry. 2012. PMID: 22399793 Free PMC article.
-
Pathogenic determinants and mechanisms of ALS/FTD linked to hexanucleotide repeat expansions in the C9orf72 gene.Neurosci Lett. 2017 Jan 1;636:16-26. doi: 10.1016/j.neulet.2016.09.007. Epub 2016 Sep 13. Neurosci Lett. 2017. PMID: 27619540 Free PMC article. Review.
-
Molecular Mechanisms of Neurodegeneration Related to C9orf72 Hexanucleotide Repeat Expansion.Behav Neurol. 2019 Jan 15;2019:2909168. doi: 10.1155/2019/2909168. eCollection 2019. Behav Neurol. 2019. PMID: 30774737 Free PMC article. Review.
Cited by
-
Frontotemporal Dementia.Neurol Clin. 2017 May;35(2):339-374. doi: 10.1016/j.ncl.2017.01.008. Neurol Clin. 2017. PMID: 28410663 Free PMC article. Review.
-
Dementia and neuroimaging.J Neurol. 2013 Feb;260(2):685-91. doi: 10.1007/s00415-012-6778-x. Epub 2012 Dec 15. J Neurol. 2013. PMID: 23241895 Review.
-
Timing and significance of pathological features in C9orf72 expansion-associated frontotemporal dementia.Brain. 2016 Dec;139(Pt 12):3202-3216. doi: 10.1093/brain/aww250. Epub 2016 Oct 22. Brain. 2016. PMID: 27797809 Free PMC article.
-
Genetic counseling for FTD/ALS caused by the C9ORF72 hexanucleotide expansion.Alzheimers Res Ther. 2012 Jul 19;4(4):27. doi: 10.1186/alzrt130. eCollection 2012. Alzheimers Res Ther. 2012. PMID: 22808918 Free PMC article. Review.
-
Young-onset dementia: scoping review of key pointers to diagnostic accuracy.BJPsych Open. 2019 Jun 4;5(3):e48. doi: 10.1192/bjo.2019.36. BJPsych Open. 2019. PMID: 31530311 Free PMC article.
References
-
- Knopman DS, Petersen RC, Edland SD, Cha RH, Rocca WA. The incidence of frontotemporal lobar degeneration in Rochester, Minnesota, 1990 through 1994. Neurology 2004;62:506–508 - PubMed
-
- Ratnavalli E, Brayne C, Dawson K, Hodges JR. The prevalence of frontotemporal dementia. Neurology 2002;58:1615–1621 - PubMed
-
- Ringholz GM, Appel SH, Bradshaw M, Cooke NA, Mosnik DM, Schulz PE. Prevalence and patterns of cognitive impairment in sporadic ALS. Neurology 2005;65:586–590 - PubMed
-
- Lomen-Hoerth C, Murphy J, Langmore S, Kramer JH, Olney RK, Miller B. Are amyotrophic lateral sclerosis patients cognitively normal? Neurology 2003;60:1094–1097 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AG026938/AG/NIA NIH HHS/United States
- R01 AG031278/AG/NIA NIH HHS/United States
- P01 AG017586/AG/NIA NIH HHS/United States
- P50AG023501/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- R01AG031278/AG/NIA NIH HHS/United States
- 1R01AG029577-01/AG/NIA NIH HHS/United States
- P50 AG1657303/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- K23 AG039414/AG/NIA NIH HHS/United States
- RC1 AG035610/AG/NIA NIH HHS/United States
- R01NS065782/NS/NINDS NIH HHS/United States
- R01AG026251/AG/NIA NIH HHS/United States
- K23AG039414-01A1/AG/NIA NIH HHS/United States
- R01AG038791/AG/NIA NIH HHS/United States
- P01AG019724/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous