

C3 glomerulonephritis: clinicopathological findings, complement abnormalities, glomerular proteomic profile, treatment, and follow-up
- PMID: 22673887
- PMCID: PMC4438675
- DOI: 10.1038/ki.2012.212
C3 glomerulonephritis: clinicopathological findings, complement abnormalities, glomerular proteomic profile, treatment, and follow-up
Abstract
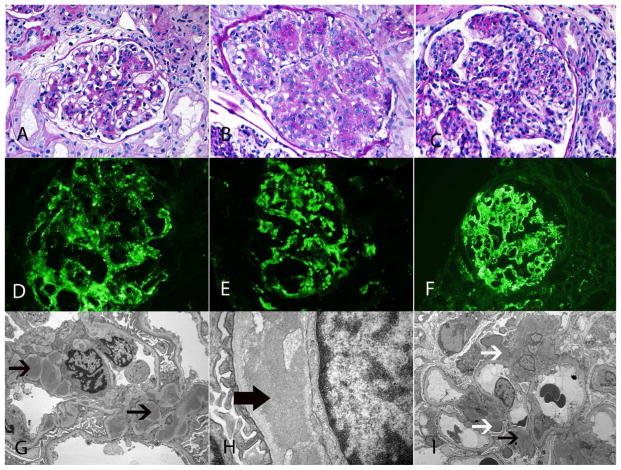
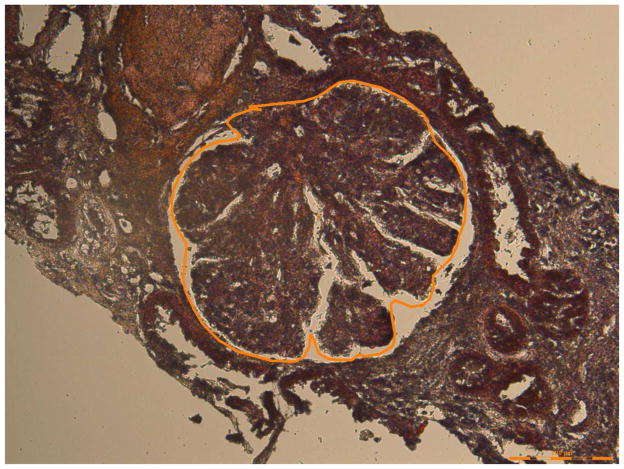
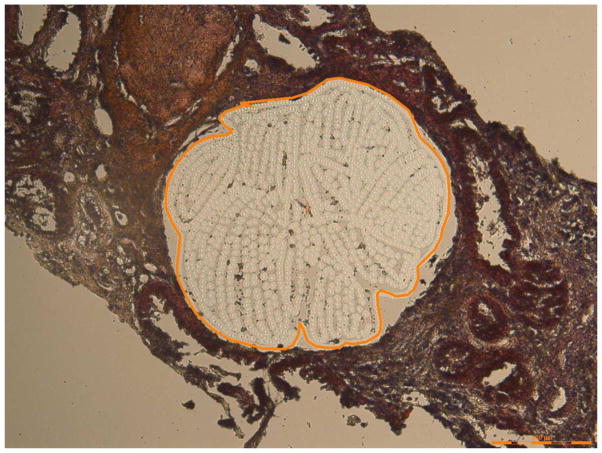
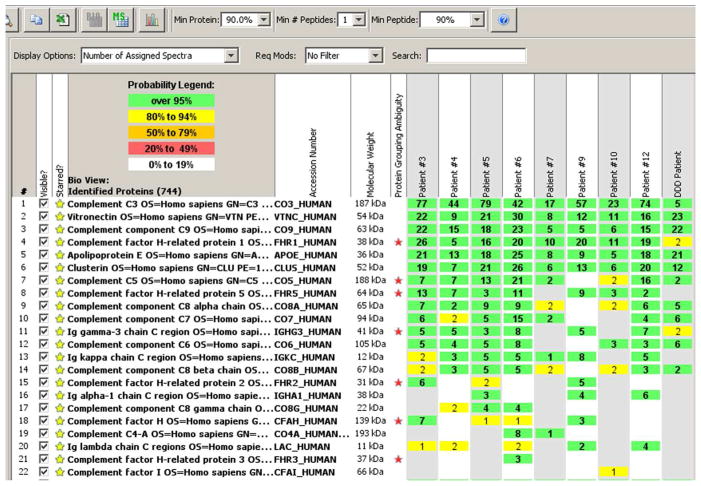
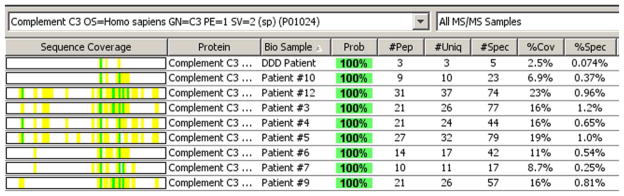
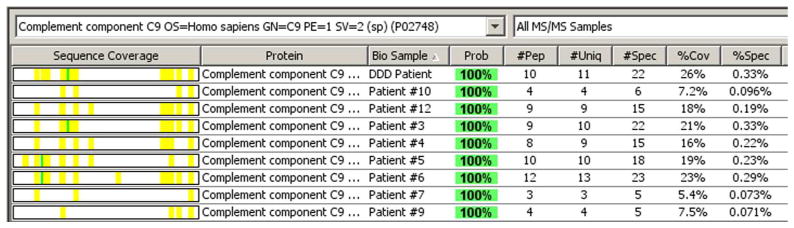
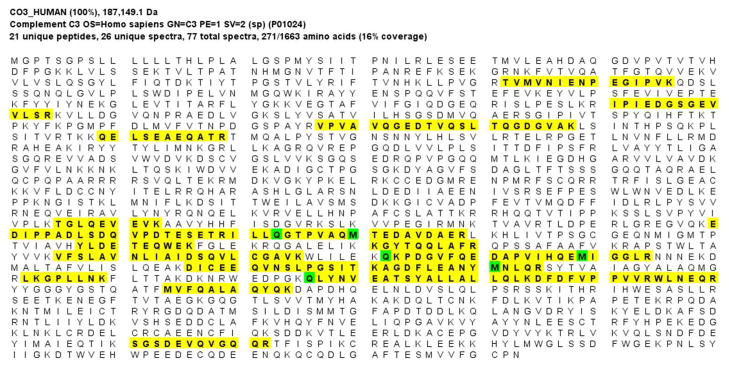
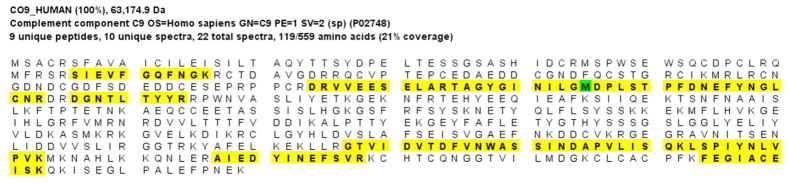
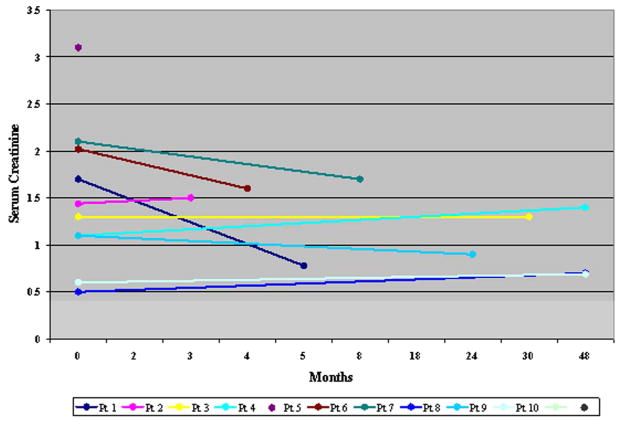
C3 glomerulonephritis (C3GN) is a recently described disorder that typically results from abnormalities in the alternative pathway (AP) of complement. Here, we describe the clinical features, kidney biopsy findings, AP abnormalities, glomerular proteomic profile, and follow-up in 12 cases of C3GN. This disorder equally affected all ages, both genders, and typically presented with hematuria and proteinuria. In both the short and long term, renal function remained stable in the majority of patients with native kidney disease. In two patients, C3GN recurred within 1 year of transplantation and resulted in a decline in allograft function. Kidney biopsy mainly showed a membranoproliferative pattern, although both mesangial proliferative and diffuse endocapillary proliferative glomerulonephritis were noted. AP abnormalities were heterogeneous, both acquired and genetic. The most common acquired abnormality was the presence of C3 nephritic factors, while the most common genetic finding was the presence of H402 and V62 alleles of Factor H. In addition to these risk factors, other abnormalities included Factor H autoantibodies and mutations in CFH, CFI, and CFHR genes. Laser dissection and mass spectrometry of glomeruli from patients with C3GN showed accumulation of AP and terminal complement complex proteins. Thus, C3GN results from diverse abnormalities of the alternative complement pathway leading to subsequent glomerular injury.
Figures
Comment in
-
Redefining C3 glomerulopathy: 'C3 only' is a bridge too far.Kidney Int. 2013 Feb;83(2):331-2. doi: 10.1038/ki.2012.385. Kidney Int. 2013. PMID: 23364589 No abstract available.
-
The author replys:Kidney Int. 2013 Feb;83(2):332. doi: 10.1038/ki.2012.380. Kidney Int. 2013. PMID: 23364591 No abstract available.
Similar articles
-
Acquired and genetic complement abnormalities play a critical role in dense deposit disease and other C3 glomerulopathies.Kidney Int. 2012 Aug;82(4):454-64. doi: 10.1038/ki.2012.63. Epub 2012 Mar 28. Kidney Int. 2012. PMID: 22456601
-
Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience.Diagn Pathol. 2015 Mar 17;10:6. doi: 10.1186/s13000-015-0233-0. Diagn Pathol. 2015. PMID: 25889427 Free PMC article.
-
Proliferative glomerulonephritis secondary to dysfunction of the alternative pathway of complement.Clin J Am Soc Nephrol. 2011 May;6(5):1009-17. doi: 10.2215/CJN.07110810. Epub 2011 Mar 17. Clin J Am Soc Nephrol. 2011. PMID: 21415311 Free PMC article.
-
C3 glomerulopathy.Contrib Nephrol. 2013;181:185-93. doi: 10.1159/000348654. Epub 2013 May 8. Contrib Nephrol. 2013. PMID: 23689580 Review.
-
Autoimmune abnormalities of the alternative complement pathway in membranoproliferative glomerulonephritis and C3 glomerulopathy.Pediatr Nephrol. 2019 Aug;34(8):1311-1323. doi: 10.1007/s00467-018-3989-0. Epub 2018 Jun 9. Pediatr Nephrol. 2019. PMID: 29948306 Review.
Cited by
-
C4d at Crossroads Between Post-Infectious Glomerulonephritis and C3 Glomerulopathy.Int J Nephrol Renovasc Dis. 2021 Mar 11;14:87-95. doi: 10.2147/IJNRD.S285302. eCollection 2021. Int J Nephrol Renovasc Dis. 2021. PMID: 33732010 Free PMC article.
-
Reclassification of membranoproliferative glomerulonephritis: Identification of a new GN: C3GN.World J Nephrol. 2016 Jul 6;5(4):308-20. doi: 10.5527/wjn.v5.i4.308. World J Nephrol. 2016. PMID: 27458560 Free PMC article. Review.
-
Clinicopathological features of C3 glomerulopathy in children: a single-center experience.Pediatr Nephrol. 2020 Jan;35(1):153-162. doi: 10.1007/s00467-019-04388-3. Epub 2019 Oct 30. Pediatr Nephrol. 2020. PMID: 31667615
-
C3-Glomerulopathy Autoantibodies Mediate Distinct Effects on Complement C3- and C5-Convertases.Front Immunol. 2019 May 31;10:1030. doi: 10.3389/fimmu.2019.01030. eCollection 2019. Front Immunol. 2019. PMID: 31214159 Free PMC article.
-
De novo glomerular diseases after renal transplantation: How is it different from recurrent glomerular diseases?World J Transplant. 2017 Dec 24;7(6):285-300. doi: 10.5500/wjt.v7.i6.285. World J Transplant. 2017. PMID: 29312858 Free PMC article. Review.
References
-
- Fakhouri F, Fremeaux-Bacchi V, Noel L-H, Cook HT, Pickering MC. C3 glomerulopathy: a new classification. Nat Rev Nephrol. 2010;6(8):494–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
