

Association of coffee drinking with total and cause-specific mortality
- PMID: 22591295
- PMCID: PMC3439152
- DOI: 10.1056/NEJMoa1112010
Association of coffee drinking with total and cause-specific mortality
Erratum in
- N Engl J Med. 2012 Jul 19;367(3):285
Abstract
Background: Coffee is one of the most widely consumed beverages, but the association between coffee consumption and the risk of death remains unclear.
Methods: We examined the association of coffee drinking with subsequent total and cause-specific mortality among 229,119 men and 173,141 women in the National Institutes of Health-AARP Diet and Health Study who were 50 to 71 years of age at baseline. Participants with cancer, heart disease, and stroke were excluded. Coffee consumption was assessed once at baseline.
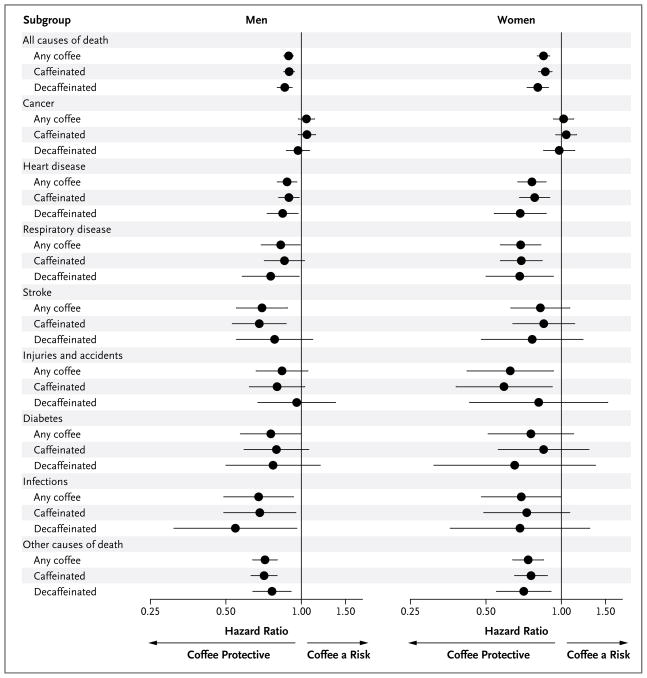
Results: During 5,148,760 person-years of follow-up between 1995 and 2008, a total of 33,731 men and 18,784 women died. In age-adjusted models, the risk of death was increased among coffee drinkers. However, coffee drinkers were also more likely to smoke, and, after adjustment for tobacco-smoking status and other potential confounders, there was a significant inverse association between coffee consumption and mortality. Adjusted hazard ratios for death among men who drank coffee as compared with those who did not were as follows: 0.99 (95% confidence interval [CI], 0.95 to 1.04) for drinking less than 1 cup per day, 0.94 (95% CI, 0.90 to 0.99) for 1 cup, 0.90 (95% CI, 0.86 to 0.93) for 2 or 3 cups, 0.88 (95% CI, 0.84 to 0.93) for 4 or 5 cups, and 0.90 (95% CI, 0.85 to 0.96) for 6 or more cups of coffee per day (P<0.001 for trend); the respective hazard ratios among women were 1.01 (95% CI, 0.96 to 1.07), 0.95 (95% CI, 0.90 to 1.01), 0.87 (95% CI, 0.83 to 0.92), 0.84 (95% CI, 0.79 to 0.90), and 0.85 (95% CI, 0.78 to 0.93) (P<0.001 for trend). Inverse associations were observed for deaths due to heart disease, respiratory disease, stroke, injuries and accidents, diabetes, and infections, but not for deaths due to cancer. Results were similar in subgroups, including persons who had never smoked and persons who reported very good to excellent health at baseline.
Conclusions: In this large prospective study, coffee consumption was inversely associated with total and cause-specific mortality. Whether this was a causal or associational finding cannot be determined from our data. (Funded by the Intramural Research Program of the National Institutes of Health, National Cancer Institute, Division of Cancer Epidemiology and Genetics.).
Figures

Comment in
-
Coffee drinking and mortality.N Engl J Med. 2012 Aug 9;367(6):575; author reply 576-7. doi: 10.1056/NEJMc1207172. N Engl J Med. 2012. PMID: 22873544 No abstract available.
-
Coffee drinking and mortality.N Engl J Med. 2012 Aug 9;367(6):575-6; author reply 576-7. doi: 10.1056/NEJMc1207172. N Engl J Med. 2012. PMID: 22873545 No abstract available.
-
Coffee drinking and mortality.N Engl J Med. 2012 Aug 9;367(6):576; author reply 576-7. doi: 10.1056/NEJMc1207172. N Engl J Med. 2012. PMID: 22873546 No abstract available.
-
Long-term coffee consumption associated with reduced risk of total and cause-specific mortality.Evid Based Med. 2013 Jun;18(3):116-7. doi: 10.1136/eb-2012-100878. Epub 2012 Aug 25. Evid Based Med. 2013. PMID: 22923704 No abstract available.
-
[Journal club].Z Gerontol Geriatr. 2012 Oct;45(7):673-4. doi: 10.1007/s00391-012-0378-3. Z Gerontol Geriatr. 2012. PMID: 23052284 German. No abstract available.
Similar articles
-
The relationship of coffee consumption with mortality.Ann Intern Med. 2008 Jun 17;148(12):904-14. doi: 10.7326/0003-4819-148-12-200806170-00003. Ann Intern Med. 2008. PMID: 18559841 Free PMC article.
-
Association of Coffee Consumption With Total and Cause-Specific Mortality Among Nonwhite Populations.Ann Intern Med. 2017 Aug 15;167(4):228-235. doi: 10.7326/M16-2472. Epub 2017 Jul 11. Ann Intern Med. 2017. PMID: 28693036 Free PMC article.
-
Association of Coffee Consumption With Overall and Cause-Specific Mortality in a Large US Prospective Cohort Study.Am J Epidemiol. 2015 Dec 15;182(12):1010-22. doi: 10.1093/aje/kwv146. Epub 2015 Nov 27. Am J Epidemiol. 2015. PMID: 26614599 Free PMC article. Clinical Trial.
-
Association of Coffee Consumption With Total and Cause-Specific Mortality in 3 Large Prospective Cohorts.Circulation. 2015 Dec 15;132(24):2305-15. doi: 10.1161/CIRCULATIONAHA.115.017341. Epub 2015 Nov 16. Circulation. 2015. PMID: 26572796 Free PMC article.
-
Coffee consumption and the risk of lung cancer: an updated meta-analysis of epidemiological studies.Eur J Clin Nutr. 2016 Feb;70(2):199-206. doi: 10.1038/ejcn.2015.96. Epub 2015 Jun 17. Eur J Clin Nutr. 2016. PMID: 26081490 Review.
Cited by
-
Additive effects of green tea and coffee on all-cause mortality in patients with type 2 diabetes mellitus: the Fukuoka Diabetes Registry.BMJ Open Diabetes Res Care. 2020 Oct;8(1):e001252. doi: 10.1136/bmjdrc-2020-001252. BMJ Open Diabetes Res Care. 2020. PMID: 33087342 Free PMC article.
-
Essential Roles of Natural Products and Gaseous Mediators on Neuronal Cell Death or Survival.Int J Mol Sci. 2016 Sep 29;17(10):1652. doi: 10.3390/ijms17101652. Int J Mol Sci. 2016. PMID: 27690018 Free PMC article. Review.
-
Association between coffee and green tea intake and pneumonia among the Japanese elderly: a case-control study.Sci Rep. 2021 Mar 10;11(1):5570. doi: 10.1038/s41598-021-84348-w. Sci Rep. 2021. PMID: 33692403 Free PMC article. Clinical Trial.
-
Coffee but not green tea consumption is associated with prevalence and severity of hepatic steatosis: the impact on leptin level.Eur J Clin Nutr. 2015 Sep;69(9):1023-7. doi: 10.1038/ejcn.2015.23. Epub 2015 Mar 25. Eur J Clin Nutr. 2015. PMID: 25804274
-
No Effects of Black Tea on Cognitive Decline Among Older US Men: A Prospective Cohort Study.J Alzheimers Dis. 2018;65(1):99-105. doi: 10.3233/JAD-180103. J Alzheimers Dis. 2018. PMID: 30040715 Free PMC article.
References
-
- Gómez-Ruiz JA, Leake DS, Ames JM. In vitro antioxidant activity of coffee compounds and their metabolites. J Agric Food Chem. 2007;55:6962–9. [Erratum, J Agric Food Chem 2007;55:8284.] - PubMed
-
- Lopez-Garcia E, van Dam RM, Qi L, Hu FB. Coffee consumption and markers of inflammation and endothelial dysfunction in healthy and diabetic women. Am J Clin Nutr. 2006;84:888–93. - PubMed
-
- Arion WJ, Canfield WK, Ramos FC, et al. Chlorogenic acid and hydroxynitrobenzaldehyde: new inhibitors of hepatic glucose 6-phosphatase. Arch Biochem Biophys. 1997;339:315–22. - PubMed
-
- Huxley R, Lee CM, Barzi F, et al. Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Arch Intern Med. 2009;169:2053–63. - PubMed
-
- Coffee drinking and acute myocardial infarction: report from the Boston Collaborative Drug Surveillance Program. Lancet. 1972;2:1278–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources