

Adjunctive interferon-γ immunotherapy for the treatment of HIV-associated cryptococcal meningitis: a randomized controlled trial
- PMID: 22421244
- PMCID: PMC3640254
- DOI: 10.1097/QAD.0b013e3283536a93
Adjunctive interferon-γ immunotherapy for the treatment of HIV-associated cryptococcal meningitis: a randomized controlled trial
Abstract
Background: Interferon-gamma (IFNγ) is of key importance in the immune response to Cryptococcus neoformans. Mortality related to cryptococcal meningitis remains high, and novel treatment strategies are needed. We performed a randomized controlled trial to determine whether addition of IFNγ to standard therapy increased the rate of clearance of cryptococcal infection in HIV-associated cryptococcal meningitis.
Methods: Patients were randomized to amphotericin B 1 mg/kg per day and 5FC 100 mg/kg per day for 2 weeks (standard therapy), standard therapy and IFNγ1b 100 μg days 1 and 3 (IFNγ two doses), or standard therapy and IFNγ1b 100 μg days 1, 3, 5, 8, 10 and 12 (IFNγ six doses). Primary outcome was rate of clearance of cryptococcus from the cerebrospinal fluid (CSF) (early fungicidal activity, EFA) calculated from serial quantitative cultures, previously shown to be independently associated with survival.
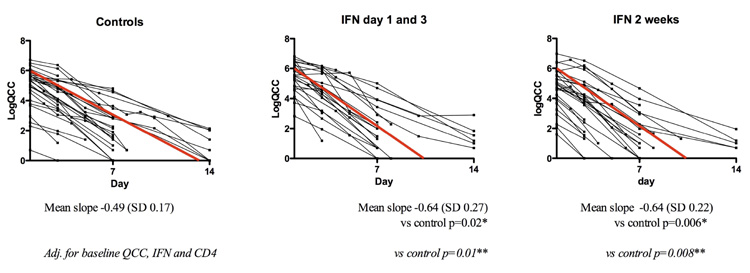
Results: Rate of fungal clearance was significantly faster in IFNγ containing groups than with standard treatment. Mean EFA [log colony forming unit (CFU)/ml per day] was -0.49 with standard treatment, -0.64 with IFNγ two doses, and -0.64 with IFNγ six doses. Difference in EFA was -0.15 [confidence interval (95% CI) -0.02 to -0.27, P=0.02] between standard treatment and IFNγ two doses, and -0.15 (95% CI -0.05 to -0.26, P=0.006) between standard treatment and IFNγ six doses. Mortality was 16% (14/88) at 2 weeks and 31% (27/87) at 10 weeks, with no significant difference between groups. All treatments were well tolerated.
Conclusion: Addition of short-course IFNγ to standard treatment significantly increased the rate of clearance of cryptococcal infection from the CSF, and was not associated with any increase in adverse events. Two doses of IFNγ are as effective as six doses.
Figures

Similar articles
-
Comparison of Early Fungicidal Activity and Mortality Between Daily Liposomal Amphotericin B and Daily Amphotericin B Deoxycholate for Cryptococcal Meningitis.Clin Infect Dis. 2025 Feb 5;80(1):153-159. doi: 10.1093/cid/ciae326. Clin Infect Dis. 2025. PMID: 38943665
-
Combination antifungal therapies for HIV-associated cryptococcal meningitis: a randomised trial.Lancet. 2004 May 29;363(9423):1764-7. doi: 10.1016/S0140-6736(04)16301-0. Lancet. 2004. PMID: 15172774 Clinical Trial.
-
High-dose amphotericin B with flucytosine for the treatment of cryptococcal meningitis in HIV-infected patients: a randomized trial.Clin Infect Dis. 2008 Jul 1;47(1):123-30. doi: 10.1086/588792. Clin Infect Dis. 2008. PMID: 18505387 Clinical Trial.
-
Treatment for HIV-associated cryptococcal meningitis.Cochrane Database Syst Rev. 2018 Jul 25;7(7):CD005647. doi: 10.1002/14651858.CD005647.pub3. Cochrane Database Syst Rev. 2018. PMID: 30045416 Free PMC article. Review.
-
Treatment of acute cryptococcal meningitis in HIV infected adults, with an emphasis on resource-limited settings.Cochrane Database Syst Rev. 2008 Oct 8;(4):CD005647. doi: 10.1002/14651858.CD005647.pub2. Cochrane Database Syst Rev. 2008. Update in: Cochrane Database Syst Rev. 2018 Jul 25;7:CD005647. doi: 10.1002/14651858.CD005647.pub3. PMID: 18843697 Updated. Review.
Cited by
-
Diagnosis and management of cryptococcal meningitis in HIV-infected adults.Clin Microbiol Rev. 2023 Dec 20;36(4):e0015622. doi: 10.1128/cmr.00156-22. Epub 2023 Nov 28. Clin Microbiol Rev. 2023. PMID: 38014977 Free PMC article. Review.
-
Adjuvant ArtinM favored the host immunity against Cryptococcus gattii infection in C57BL/6 mice.Immunotherapy. 2024;16(11):733-748. doi: 10.1080/1750743X.2024.2360384. Epub 2024 Jun 28. Immunotherapy. 2024. PMID: 38940276
-
AMBITION-cm: intermittent high dose AmBisome on a high dose fluconazole backbone for cryptococcal meningitis induction therapy in sub-Saharan Africa: study protocol for a randomized controlled trial.Trials. 2015 Jun 17;16:276. doi: 10.1186/s13063-015-0799-6. Trials. 2015. PMID: 26081985 Free PMC article. Clinical Trial.
-
Superficial Dermatophytosis across the World's Populations: Potential Benefits from Nanocarrier-Based Therapies and Rising Challenges.ACS Omega. 2023 Aug 22;8(35):31575-31599. doi: 10.1021/acsomega.3c01988. eCollection 2023 Sep 5. ACS Omega. 2023. PMID: 37692246 Free PMC article. Review.
-
Population Pharmacokinetic Model and Meta-analysis of Outcomes of Amphotericin B Deoxycholate Use in Adults with Cryptococcal Meningitis.Antimicrob Agents Chemother. 2018 Jun 26;62(7):e02526-17. doi: 10.1128/AAC.02526-17. Print 2018 Jul. Antimicrob Agents Chemother. 2018. PMID: 29735567 Free PMC article.
References
-
- Jarvis JN, Harrison TS. HIV-associated cryptococcal meningitis. Aids. 2007;21:2119–2129. - PubMed
-
- Bicanic T, Meintjes G, Wood R, Hayes M, Rebe K, Bekker LG, Harrison T. Fungal burden, early fungicidal activity, and outcome in cryptococcal meningitis in antiretroviral-naive or antiretroviral-experienced patients treated with amphotericin B or fluconazole. Clin Infect Dis. 2007;45:76–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
