

Neurological complications in HIV
- PMID: 22268312
- PMCID: PMC4952339
- DOI: 10.7861/clinmedicine.11-6-571
Neurological complications in HIV
Abstract
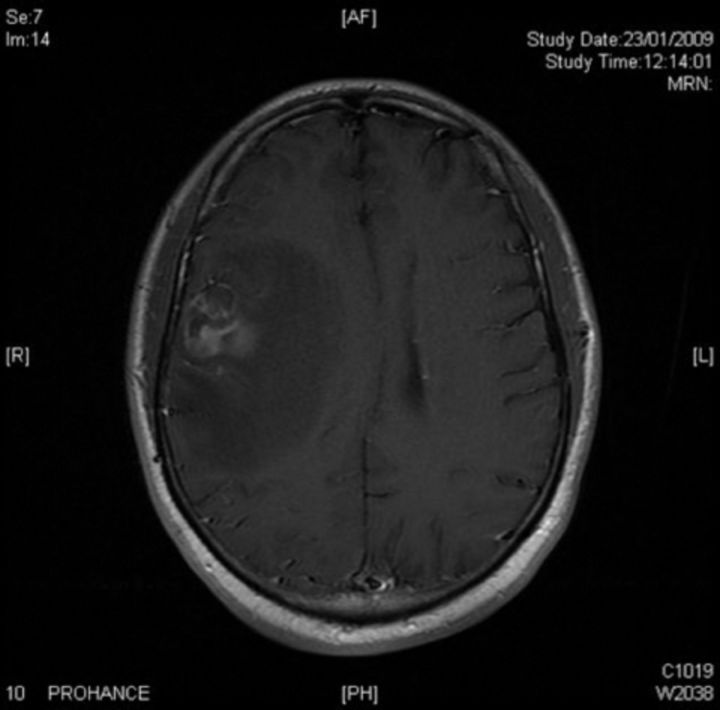
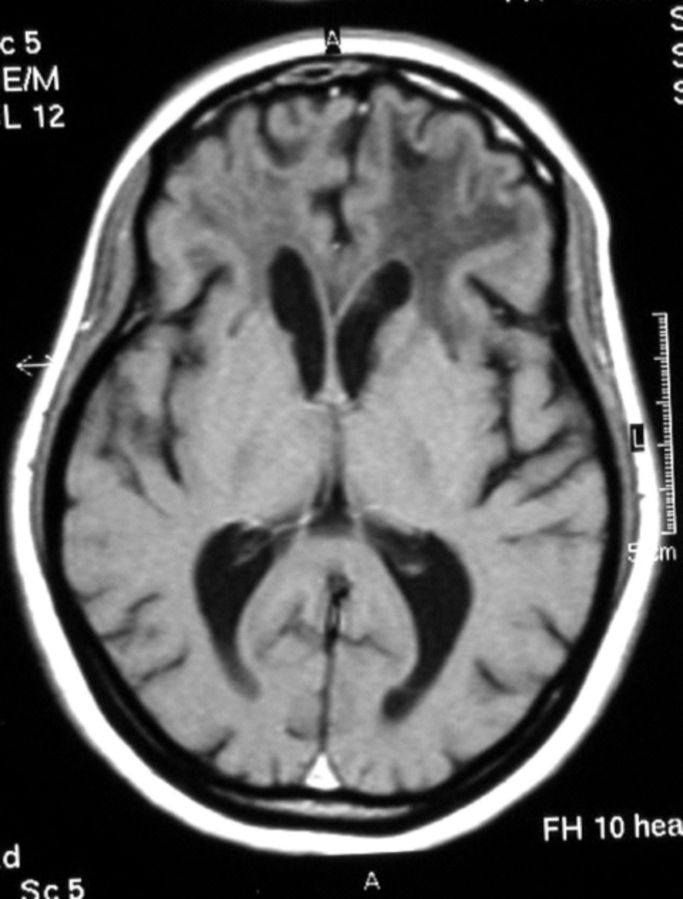
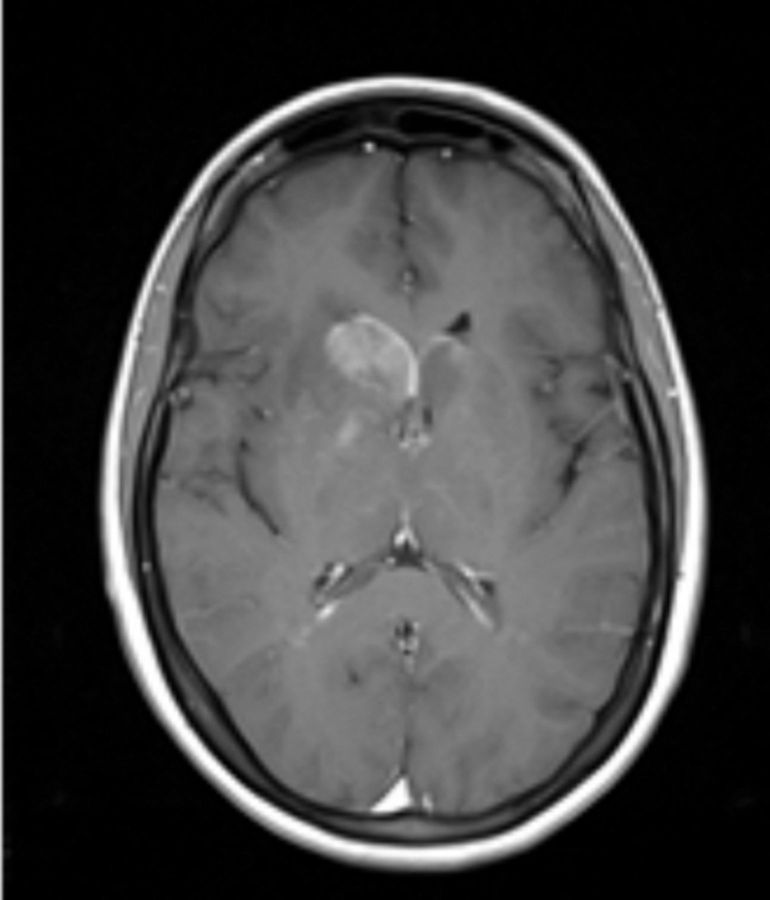
HIV is neuroinvasive with early involvement of the nervous system and has the potential to cause disease at any site of the neuro-axis during the evolution from seroconversion to late stage HIV. Disease may result from direct viral infection, indirect immune-deficiency driven opportunistic infections, AIDS-defining cancers, antiretroviral (ARV) drug therapy, or less well elucidated associations, such as vascular events (Table 1). Recognition of each of these is paramount in the prevention or attenuation of long-term morbidity. Though the epidemiology of neurological disease has altered substantially since the arrival of combination antiretroviral therapy (cART), with reduced incidence and improved survival, the spectrum of central nervous system (CNS) diseases has remained relatively unchanged. Despite available treatment options, mortality remains high and the morbidity significant. CNS diseases can result in long hospital stays, reduced quality of life and marked disability. The majority of disease occurs in the advanced stages of HIV infection where immunosuppression is the predominant influence. Diagnosis can prove challenging as presentation is often atypical and there can be significant neurological involvement with limited evidence of disease. Multiple aetiologies can co-exist and investigations may yield unexpected results, rendering interpretation difficult. Paradoxically, cART may also alter the way CNS disease manifests and unmask opportunistic infections or cause clinical representation of the opportunistic infections, when it represents immune reconstitution syndrome (IRS). Clinical assessment, imaging (typically magnetic resonance imaging (MRI)) and cerebral spinal fluid (CSF) sampling remain the chief diagnostic tools. This conference summary reviews these differing aspects.
Figures
Similar articles
-
HIV-Associated Neurologic Disorders and Central Nervous System Opportunistic Infections in HIV.Semin Neurol. 2016 Aug;36(4):373-81. doi: 10.1055/s-0036-1585454. Epub 2016 Sep 19. Semin Neurol. 2016. PMID: 27643907 Review.
-
Imaging of pediatric central nervous system HIV infection.Neuroimaging Clin N Am. 1997 May;7(2):321-39. Neuroimaging Clin N Am. 1997. PMID: 9113693 Review.
-
[Magnetic resonance imaging findings of the brain in adult HIV and AIDS patients].Rofo. 2008 Jan;180(1):21-9. doi: 10.1055/s-2007-963567. Epub 2007 Nov 16. Rofo. 2008. PMID: 18008191 Review. German.
-
Common neurologic complications of HIV-1 infection and AIDS.Am Fam Physician. 1995 Feb 1;51(2):387-98. Am Fam Physician. 1995. PMID: 7840035 Review.
-
Neurological disorders in HIV in Africa: a review.Afr Health Sci. 2019 Jun;19(2):1953-1977. doi: 10.4314/ahs.v19i2.19. Afr Health Sci. 2019. PMID: 31656479 Free PMC article. Review.
Cited by
-
Neurological Disorders of Patients Living with HIV Hospitalized in Infectious Departments of the Specialist Hospital in Lower Silesia in Poland.Healthcare (Basel). 2022 Aug 7;10(8):1481. doi: 10.3390/healthcare10081481. Healthcare (Basel). 2022. PMID: 36011138 Free PMC article.
-
Understanding HIV-associated neurocognitive and neurodegenerative disorders (neuroAIDS): enroute to achieve the 95-95-95 target and sustainable development goal for HIV/AIDS response.Virusdisease. 2023 Jun;34(2):165-171. doi: 10.1007/s13337-023-00830-1. Epub 2023 Jun 26. Virusdisease. 2023. PMID: 37408553 Free PMC article. Review.
-
Persistent metabolic changes in HIV-infected patients during the first year of combination antiretroviral therapy.Sci Rep. 2018 Nov 16;8(1):16947. doi: 10.1038/s41598-018-35271-0. Sci Rep. 2018. PMID: 30446683 Free PMC article.
-
Peripheral neuropathy in primary HIV infection associates with systemic and central nervous system immune activation.J Acquir Immune Defic Syndr. 2014 Jul 1;66(3):303-10. doi: 10.1097/QAI.0000000000000167. J Acquir Immune Defic Syndr. 2014. PMID: 24732871 Free PMC article.
-
Idiopathic Intracranial Hypertension in an Adolescent With Recent Human Immunodeficiency Virus (HIV) Diagnosis: A Challenging Etiological Dilemma.Cureus. 2024 May 9;16(5):e60001. doi: 10.7759/cureus.60001. eCollection 2024 May. Cureus. 2024. PMID: 38854218 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
