

Failure to normalize lymphopenia following trauma is associated with increased mortality, independent of the leukocytosis pattern
- PMID: 22264310
- PMCID: PMC3396248
- DOI: 10.1186/cc11157
Failure to normalize lymphopenia following trauma is associated with increased mortality, independent of the leukocytosis pattern
Abstract
Introduction: Following trauma and systemic inflammatory response syndrome (SIRS), the typical response is an elevation of the total complete blood count (CBC) and a reduction of the lymphocyte count. This leukocytosis typically returns to normal within 48 hours. The persistence of a leukocytosis following trauma is associated with adverse outcomes. Although lymphocyte anergy and dysfunction following trauma is associated with increased risk for infection and sepsis, there is a paucity of data regarding the impact of a persistence of a low lymphocyte count in trauma patients.
Methods: This is a retrospective review of prospectively collected data from trauma patients collected over the 5 years of September 2003 to September 2008. Patients were included if the injury severity score (ISS) was >or=15, and they survived at least 3 days. Demographic data, mechanism and injury severity score, mortality, and length of stay were collected from the medical record. Laboratory values for the first 4 hospital days were collected. Leukocyte, neutrophil and lymphocyte counts were extracted from the daily complete blood count (CBC). Patients were then grouped based on response (elevation/depression) of each component of the CBC, and their return, or failure thereof, to normal. Proportional hazards regression with time-varying covariates as well as Kaplan-Meier curves were used to predict risk of death, time to death and time to healthy discharge based on fluctuations of the individual components of the CBC.
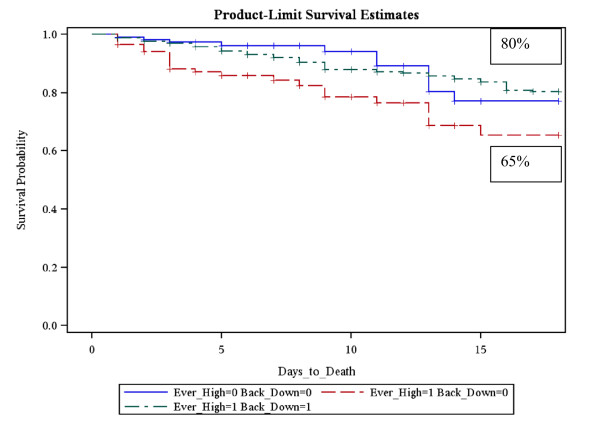
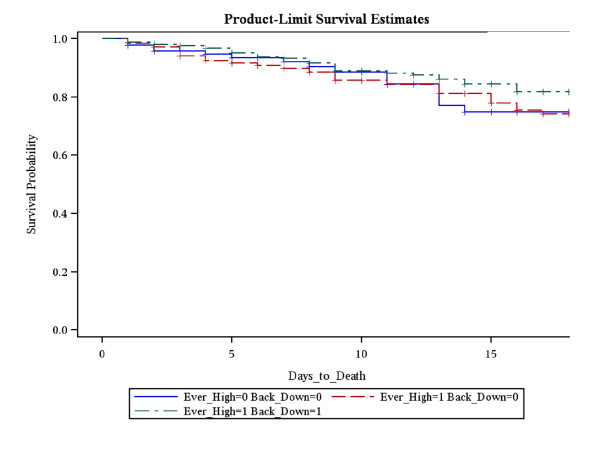
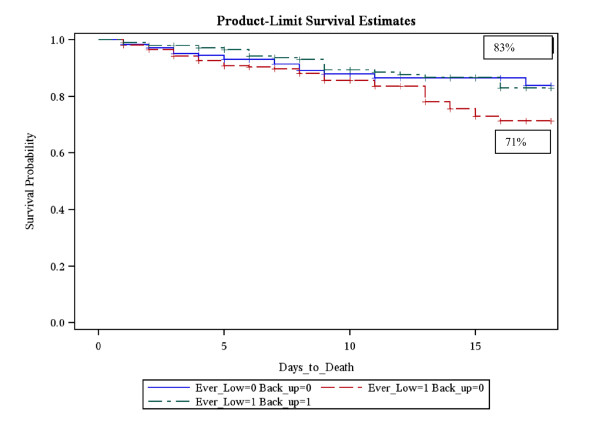
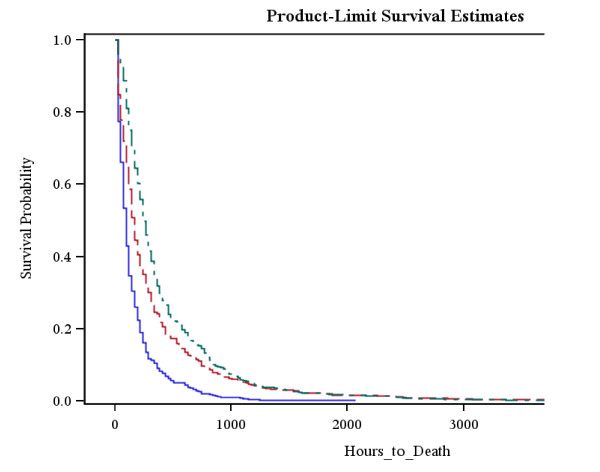
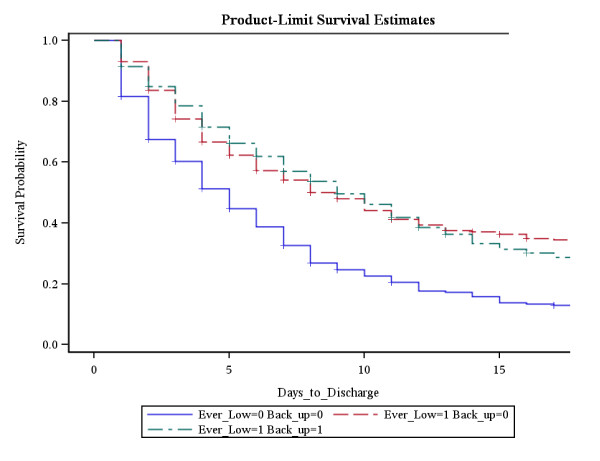
Results: There were 2448 patients admitted over the 5 years included in the analysis. When adjusting for age, gender and ISS the relative risk of death was elevated with a persistent leukocytosis (2.501 (95% CI=1.477-4.235)) or failure to normalize lymphopenia (1.639 (95% CI=10.17-2.643)) within the first 4 days following admission. Similar results were seen when Kaplan-Meier curves were created. Persistent lymphopenia was associated with shortest time to death. Paradoxically in survivors persistent lymphopenia was associated with the shortest time to discharge.
Conclusions: Persistently abnormal CBC responses are associated with a higher mortality following trauma. This is the first report noting that a failure to normalize lymphopenia in severely injured patients is associated with significantly higher mortality.
Figures
Comment in
-
CD4+ T-lymphocyte alterations in trauma patients.Crit Care. 2012 Jun 26;16(3):432. doi: 10.1186/cc11376. Crit Care. 2012. PMID: 22734607 Free PMC article. No abstract available.
Similar articles
-
CD4+ T-lymphocyte alterations in trauma patients.Crit Care. 2012 Jun 26;16(3):432. doi: 10.1186/cc11376. Crit Care. 2012. PMID: 22734607 Free PMC article. No abstract available.
-
[Early changes within the lymphocyte population are associated with the long term prognosis in severely injured patients].Beijing Da Xue Xue Bao Yi Xue Ban. 2022 Jun 18;54(3):552-556. doi: 10.19723/j.issn.1671-167X.2022.03.023. Beijing Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35701135 Free PMC article. Chinese.
-
Persistent lymphopenia after diagnosis of sepsis predicts mortality.Shock. 2014 Nov;42(5):383-91. doi: 10.1097/SHK.0000000000000234. Shock. 2014. PMID: 25051284 Free PMC article.
-
Persistent lymphopenia is an independent predictor of mortality in critically ill emergency general surgical patients.Eur J Trauma Emerg Surg. 2016 Dec;42(6):755-760. doi: 10.1007/s00068-015-0585-x. Epub 2015 Oct 26. Eur J Trauma Emerg Surg. 2016. PMID: 26501197
-
Back to basics: validation of the admission systemic inflammatory response syndrome score in predicting outcome in trauma.J Trauma. 2001 Sep;51(3):458-63. doi: 10.1097/00005373-200109000-00006. J Trauma. 2001. PMID: 11535891
Cited by
-
Clinical predictive value of the initial neutrophils to lymphocytes and platelets ratio for prognosis of sepsis patients in the intensive care unit: a retrospective study.Front Med (Lausanne). 2024 Jan 18;11:1351492. doi: 10.3389/fmed.2024.1351492. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38318247 Free PMC article.
-
Early changes within the lymphocyte population are associated with the development of multiple organ dysfunction syndrome in trauma patients.Crit Care. 2016 Jun 7;20(1):176. doi: 10.1186/s13054-016-1341-2. Crit Care. 2016. PMID: 27268230 Free PMC article.
-
Preoperative Controlling Nutritional Status Score on Predicting the Postoperative Complications Following Major Hepatopancreatobiliary Surgery.Cureus. 2024 May 30;16(5):e61349. doi: 10.7759/cureus.61349. eCollection 2024 May. Cureus. 2024. PMID: 38947640 Free PMC article.
-
The immune response to surgery and infection.Cent Eur J Immunol. 2014;39(4):532-7. doi: 10.5114/ceji.2014.47741. Epub 2014 Dec 15. Cent Eur J Immunol. 2014. PMID: 26155175 Free PMC article. Review.
-
Diagnostic Performance of Neutrophil to Lymphocyte Ratio, Monocyte to Lymphocyte Ratio, Platelet to Lymphocyte Ratio, and Platelet to Mean Platelet Volume Ratio in Periprosthetic Hip and Knee Infections: A Systematic Review and Meta-Analysis.Diagnostics (Basel). 2022 Aug 23;12(9):2033. doi: 10.3390/diagnostics12092033. Diagnostics (Basel). 2022. PMID: 36140435 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
