

Acetazolamide improves loop gain but not the other physiological traits causing obstructive sleep apnoea
- PMID: 22219335
- PMCID: PMC3381825
- DOI: 10.1113/jphysiol.2011.223925
Acetazolamide improves loop gain but not the other physiological traits causing obstructive sleep apnoea
Abstract
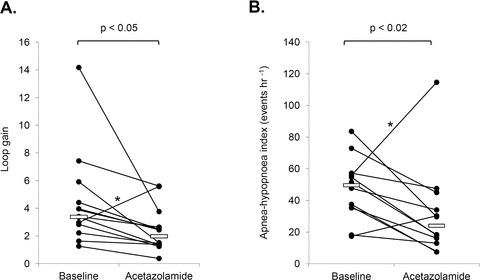
There is some evidence to suggest that acetazolamide may improve obstructive sleep apnoea (OSA).However, how acetazolamide affects the key traits causing OSA remains uncertain. We aimed to investigate the effect of acetazolamide on the traits contributing to OSA and its severity. Acetazolamide (500 mg twice daily) was administered for 1 week to 13 OSA subjects. Pharyngeal anatomy/collapsibility, loop gain (LG), upper-airway muscle responsiveness (gain) and the arousal threshold were determined using multiple 3 min 'CPAP pressure drops': pharyngeal anatomy/collapsibility was quantified as the ventilation at CPAP=0. LG was defined as the ratio of the ventilatory overshoot to the preceding reduction in ventilation. Upper-airway gain was taken as the ratio of the increase in ventilation to the increase in ventilatory drive across the drop. Arousal threshold was quantified as the level of ventilatory drive associated with arousal. The apnoea-hypopnoea index (AHI)was assessed on separate nights using standard polysomnography. Acetazolamide reduced the median [interquartile range] LG (3.4 [2.4-5.4] versus 2.0 [1.4-3.5]; P <0.05) and NREM AHI (50 [36-57] versus 24 [13-42] events h-1; P <0.05), but did not significantly alter pharyngeal anatomy/collapsibility, upper-airway gain, or arousal threshold. There was a modest correlation between the percentage reduction in LG and the percentage reduction in AHI (r =0.660, P =0.05). Our findings suggest that acetazolamide can improve OSA, probably due to reductions in the sensitivity of the ventilatory control system. Identification of patients who may benefit from reductions in LG alone or in combination with other therapies to alter the remaining traits may facilitate pharmacological resolution of OSA in the future.
Figures
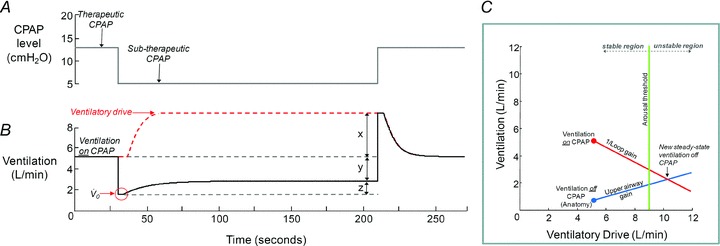
 ), upper airway gain (z/x), loop gain (x/y) and arousal threshold (if an arousal occurs); see text for details. C depicts how these four traits can be incorporated into a model to predict the susceptibility towards OSA. In this example, the new steady state (the intersection of the diagonal lines) occurs in the unstable region (i.e. right of the arousal threshold) and thus OSA is predicted to be present.
), upper airway gain (z/x), loop gain (x/y) and arousal threshold (if an arousal occurs); see text for details. C depicts how these four traits can be incorporated into a model to predict the susceptibility towards OSA. In this example, the new steady state (the intersection of the diagonal lines) occurs in the unstable region (i.e. right of the arousal threshold) and thus OSA is predicted to be present.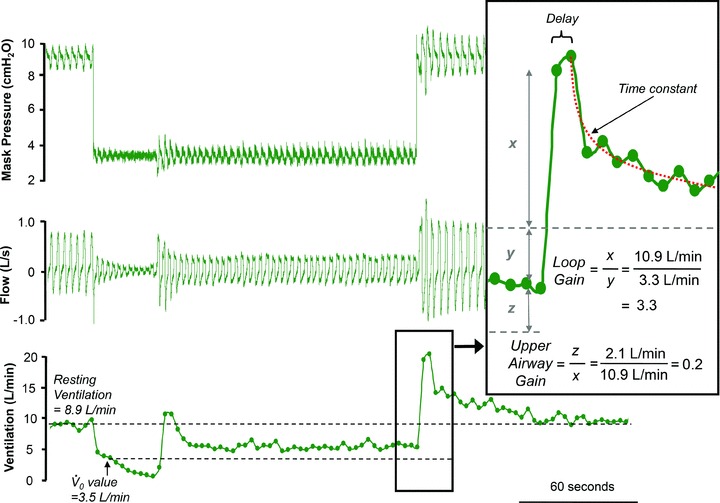
 , minute ventilation immediately after the drop is plotted on a graph against mask pressure. To estimate LG, the overshoot in ventilation (x) is divided by the amount ventilation was reduced (y). In this example, LG (x/y) is 3.3 and the upper airway gain (z/x) is +0.2 (inset panel). A delay and time constant is also calculated from the ventilatory overshoot which is used for the calculation of ventilatory drive and dynamic LG (see Supplemental Material). In this example, there was no EEG arousal, such that this drop could not be used to determine arousal threshold.
, minute ventilation immediately after the drop is plotted on a graph against mask pressure. To estimate LG, the overshoot in ventilation (x) is divided by the amount ventilation was reduced (y). In this example, LG (x/y) is 3.3 and the upper airway gain (z/x) is +0.2 (inset panel). A delay and time constant is also calculated from the ventilatory overshoot which is used for the calculation of ventilatory drive and dynamic LG (see Supplemental Material). In this example, there was no EEG arousal, such that this drop could not be used to determine arousal threshold.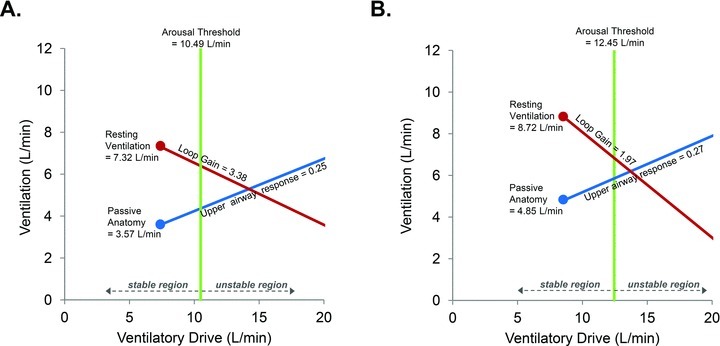
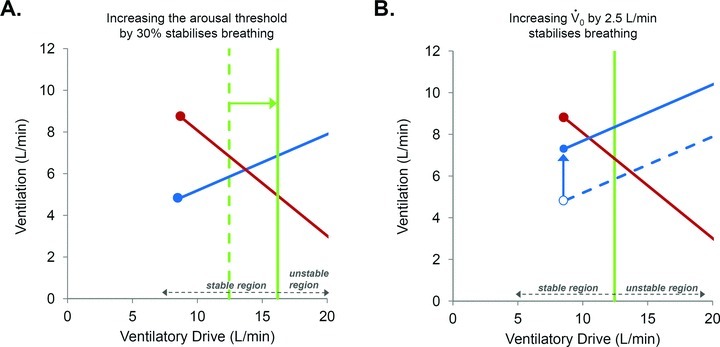
 can be improved by approximately 2.5 l min−1 with weight loss (B), then the model predicts that this would move the steady-state intersection to the left of the arousal threshold and into the stable region (i.e. stable breathing is now possible). Therefore, our model allows us to speculate that such combination therapy could achieve a complete resolution of OSA.
can be improved by approximately 2.5 l min−1 with weight loss (B), then the model predicts that this would move the steady-state intersection to the left of the arousal threshold and into the stable region (i.e. stable breathing is now possible). Therefore, our model allows us to speculate that such combination therapy could achieve a complete resolution of OSA.Comment in
-
New insights from the measurement of loop gain in obstructive sleep apnoea.J Physiol. 2012 Apr 15;590(8):1781-2. doi: 10.1113/jphysiol.2012.228643. J Physiol. 2012. PMID: 22532646 Free PMC article. No abstract available.
Similar articles
-
Acetazolamide attenuates the ventilatory response to arousal in patients with obstructive sleep apnea.Sleep. 2013 Feb 1;36(2):281-5. doi: 10.5665/sleep.2390. Sleep. 2013. PMID: 23372276 Free PMC article. Clinical Trial.
-
Effects of hyperoxia and hypoxia on the physiological traits responsible for obstructive sleep apnoea.J Physiol. 2014 Oct 15;592(20):4523-35. doi: 10.1113/jphysiol.2014.277210. Epub 2014 Aug 1. J Physiol. 2014. PMID: 25085887 Free PMC article.
-
Obstructive sleep apnea in older adults is a distinctly different physiological phenotype.Sleep. 2014 Jul 1;37(7):1227-36. doi: 10.5665/sleep.3844. Sleep. 2014. PMID: 25061251 Free PMC article.
-
Drug therapy for obstructive sleep apnoea in adults.Cochrane Database Syst Rev. 2006 Apr 19;(2):CD003002. doi: 10.1002/14651858.CD003002.pub2. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2013 May 31;(5):CD003002. doi: 10.1002/14651858.CD003002.pub3. PMID: 16625567 Updated. Review.
-
Pharmacotherapy for obstructive sleep apnea: targeting specific pathophysiological traits.Expert Rev Respir Med. 2023 Jul-Dec;17(8):663-673. doi: 10.1080/17476348.2023.2241353. Epub 2023 Aug 30. Expert Rev Respir Med. 2023. PMID: 37646222 Review.
Cited by
-
Model for Identifying High Carotid Body Chemosensitivity in Patients with Obstructive Sleep Apnea.Nat Sci Sleep. 2021 Apr 21;13:493-501. doi: 10.2147/NSS.S299646. eCollection 2021. Nat Sci Sleep. 2021. PMID: 33911906 Free PMC article.
-
Clinical Use of Loop Gain Measures to Determine Continuous Positive Airway Pressure Efficacy in Patients with Complex Sleep Apnea. A Pilot Study.Ann Am Thorac Soc. 2015 Sep;12(9):1351-7. doi: 10.1513/AnnalsATS.201410-469BC. Ann Am Thorac Soc. 2015. PMID: 26214564 Free PMC article.
-
Inherent vs. Induced Loop Gain Abnormalities in Obstructive Sleep Apnea.Front Neurol. 2018 Nov 2;9:896. doi: 10.3389/fneur.2018.00896. eCollection 2018. Front Neurol. 2018. PMID: 30450076 Free PMC article. Review.
-
Model-based estimation of loop gain using spontaneous breathing: a validation study.Respir Physiol Neurobiol. 2014 Sep 15;201:84-92. doi: 10.1016/j.resp.2014.07.002. Epub 2014 Jul 17. Respir Physiol Neurobiol. 2014. PMID: 25038522 Free PMC article.
-
The influence of head-of-bed elevation in patients with obstructive sleep apnea.Sleep Breath. 2017 Dec;21(4):815-820. doi: 10.1007/s11325-017-1524-3. Epub 2017 Jun 24. Sleep Breath. 2017. PMID: 28647854 Free PMC article. Clinical Trial.
References
-
- AASM; ESRS; JSSR; LASS. International Classification of Sleep Disorders, Revised: Diagnostic and Coding Manual. American Academy of Sleep Medicine; 2001.
-
- Bashir Y, Kann M, Stradling JR. The effect of acetazolamide on hypercapnic and eucapnic/poikilocapnic hypoxic ventilatory responses in normal subjects. Pulm Pharmacol. 1990;3:151–154. - PubMed
-
- Cherniack NS. Respiratory dysrhythmias during sleep. New Engl J Med. 1981;305:325–330. - PubMed
-
- Eckert DJ, Owens RL, Kehlmann GB, Wellman A, Rahangdale S, Yim-Yeh S, White DP, Malhotra A. Eszopiclone increases the respiratory arousal threshold and lowers the apnoea/hypopnoea index in obstructive sleep apnoea patients with a low arousal threshold. Clin Sci (Lond) 2011;120:505–514. - PMC - PubMed
-
- Edwards BA, Eckert DJ, Jordan AS, Malhotra A, Hess L, Stevenson K, White DP, Wellman A. Effect of acetazolamide in obstructive sleep apnea. Am J Respir Crit Care Med. 2010;181:A4199.
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL090897-01A2/HL/NHLBI NIH HHS/United States
- R01 HL090897/HL/NHLBI NIH HHS/United States
- R01 HL085188/HL/NHLBI NIH HHS/United States
- 5R01HL048531-16/HL/NHLBI NIH HHS/United States
- K24 HL 093218-01A1/HL/NHLBI NIH HHS/United States
- K24 HL093218/HL/NHLBI NIH HHS/United States
- R01 HL048531/HL/NHLBI NIH HHS/United States
- P01 HL095491/HL/NHLBI NIH HHS/United States
- R01 HL102321/HL/NHLBI NIH HHS/United States
- P01 HL 095491/HL/NHLBI NIH HHS/United States
- R01 HL085188-02/HL/NHLBI NIH HHS/United States
- R01 HL102321-01A1/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources