

Contributions of brain insulin resistance and deficiency in amyloid-related neurodegeneration in Alzheimer's disease
- PMID: 22191795
- PMCID: PMC4550303
- DOI: 10.2165/11597760-000000000-00000
Contributions of brain insulin resistance and deficiency in amyloid-related neurodegeneration in Alzheimer's disease
Abstract
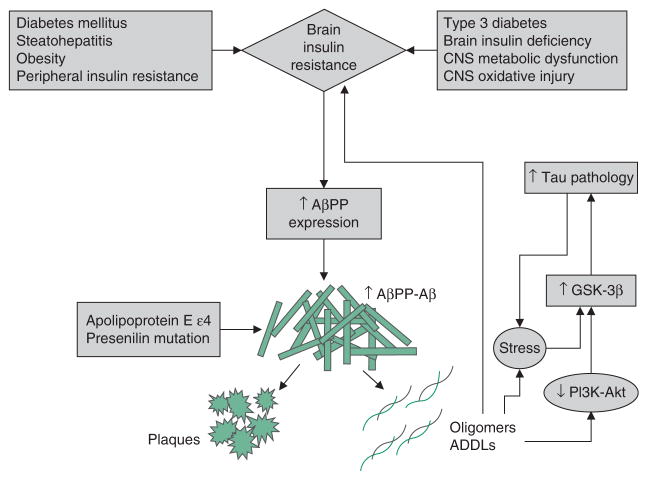
Alzheimer's disease (AD) is the most common cause of dementia in North America. Growing evidence supports the concept that AD is fundamentally a metabolic disease that results in progressive impairment in the brain's capacity to utilize glucose and respond to insulin and insulin-like growth factor (IGF) stimulation. Moreover, the heterogeneous nature of AD is only partly explained by the brain's propensity to accumulate aberrantly processed, misfolded and aggregated oligomeric structural proteins, including amyloid-β peptides and hyperphosphorylated tau. Evidence suggests that other factors, including impaired energy metabolism, oxidative stress, neuroinflammation, insulin and IGF resistance, and insulin/IGF deficiency in the brain should be incorporated into an overarching hypothesis to develop more realistic diagnostic and therapeutic approaches to AD. In this review, the interrelationship between impaired insulin and IGF signalling and amyloid-β pathology is discussed along with potential therapeutic approaches. Impairments in brain insulin/IGF signalling lead to increased expression of amyloid-β precursor protein (AβPP) and accumulation of AβPP-Aβ. In addition, they promote oxidative stress and deficits in energy metabolism, leading to the activation of pro-AβPP-Aβ-mediated neurodegeneration cascades. Although brain insulin/IGF resistance and deficiency can be induced by primary or secondary disease processes, the soaring rates of peripheral insulin resistance associated with obesity, diabetes mellitus and metabolic syndrome quite likely play major roles in the current AD epidemic. Both clinical and experimental data have linked chronic hyperinsulinaemia to cognitive impairment and neurodegeneration with increased AβPP-Aβ accumulation/reduced clearance in the CNS. Correspondingly, both the restoration of insulin responsiveness and the use of insulin therapy can lead to improved cognitive performance, although with variable effects on brain AβPP-Aβ load. On the other hand, experimental evidence supports the concept that the toxic effects of AβPP-Aβ can promote insulin resistance. Together, these findings suggest that a positive feedback loop of progressive neurodegeneration can develop whereby insulin resistance drives AβPP-Aβ accumulation, and AβPP-Aβ fibril toxicity drives brain insulin resistance. This phenomenon could explain why measuring AβPP-Aβ levels in cerebrospinal fluid or imaging of the brain has proven to be inadequate as a stand-alone biomarker for diagnosing AD, and why the clinical trial results of anti-AβPP-Aβ monotherapy have been disappointing. Instead, the aggregate data suggest that brain insulin resistance and deficiency must also be therapeutically targeted to halt AD progression or reverse its natural course. The positive therapeutic effects of different treatments that address the role of brain insulin/IGF resistance and deficiency, including the use of intranasal insulin delivery, incretins and insulin sensitizer agents are discussed along with potential benefits of lifestyle changes to modify risk for developing mild cognitive impairment or AD. Altogether, the data strongly support the notion that we must shift toward the implementation of multimodal rather than unimodal diagnostic and therapeutic strategies for AD.
Conflict of interest statement
The author has no conflicts of interest that are directly relevant to the content of this review.
Figures
Similar articles
-
Brain insulin resistance and deficiency as therapeutic targets in Alzheimer's disease.Curr Alzheimer Res. 2012 Jan;9(1):35-66. doi: 10.2174/156720512799015037. Curr Alzheimer Res. 2012. PMID: 22329651 Free PMC article. Review.
-
Brain metabolic dysfunction at the core of Alzheimer's disease.Biochem Pharmacol. 2014 Apr 15;88(4):548-59. doi: 10.1016/j.bcp.2013.12.012. Epub 2013 Dec 28. Biochem Pharmacol. 2014. PMID: 24380887 Free PMC article. Review.
-
Insulin and insulin-like growth factor expression and function deteriorate with progression of Alzheimer's disease: link to brain reductions in acetylcholine.J Alzheimers Dis. 2005 Dec;8(3):247-68. doi: 10.3233/jad-2005-8304. J Alzheimers Dis. 2005. PMID: 16340083
-
ACH2.0/E, the Consolidated Theory of Conventional and Unconventional Alzheimer's Disease: Origins, Progression, and Therapeutic Strategies.Int J Mol Sci. 2024 May 30;25(11):6036. doi: 10.3390/ijms25116036. Int J Mol Sci. 2024. PMID: 38892224 Free PMC article. Review.
-
Next Generation Therapeutic Strategy for Treatment and Prevention of Alzheimer's Disease and Aging-Associated Cognitive Decline: Transient, Once-in-a-Lifetime-Only Depletion of Intraneuronal Aβ (iAβ) by Its Targeted Degradation via Augmentation of Intra-iAβ-Cleaving Activities of BACE1 and/or BACE2.Int J Mol Sci. 2023 Dec 18;24(24):17586. doi: 10.3390/ijms242417586. Int J Mol Sci. 2023. PMID: 38139415 Free PMC article.
Cited by
-
The Angiotensin II Type 2 Receptor in Brain Functions: An Update.Int J Hypertens. 2012;2012:351758. doi: 10.1155/2012/351758. Epub 2012 Dec 25. Int J Hypertens. 2012. PMID: 23320146 Free PMC article.
-
Fundamental role of pan-inflammation and oxidative-nitrosative pathways in neuropathogenesis of Alzheimer's disease.Am J Neurodegener Dis. 2016 Mar 1;5(1):1-28. eCollection 2016. Am J Neurodegener Dis. 2016. Retraction in: Am J Neurodegener Dis. 2016 Jul 06;5(3):152. PMID: 27073740 Free PMC article. Retracted. Review.
-
Adenovirus-Mediated Transduction of Insulin-Like Growth Factor 1 Protects Hippocampal Neurons from the Toxicity of Aβ Oligomers and Prevents Memory Loss in an Alzheimer Mouse Model.Mol Neurobiol. 2020 Mar;57(3):1473-1483. doi: 10.1007/s12035-019-01827-y. Epub 2019 Nov 23. Mol Neurobiol. 2020. PMID: 31760608 Free PMC article.
-
The Full Spectrum of Alzheimer's Disease Is Rooted in Metabolic Derangements That Drive Type 3 Diabetes.Adv Exp Med Biol. 2019;1128:45-83. doi: 10.1007/978-981-13-3540-2_4. Adv Exp Med Biol. 2019. PMID: 31062325 Free PMC article. Review.
-
Alzheimer Disease Pathology and Neurodegeneration in Midlife Obesity: A Pilot Study.Aging Dis. 2024 Aug 1;15(4):1843-1854. doi: 10.14336/AD.2023.0707. Aging Dis. 2024. PMID: 37548931 Free PMC article.
References
-
- Cummings JL. Definitions and diagnostic criteria. In: Gauthier S, editor. Clinical diagnosis and management of Alzheimer’s disease. 3. London: Informa UK Limited; 2007.
-
- DeKosky ST, Carrillo MC, Phelps C, et al. Revision of the criteria for Alzheimer’s disease: a symposium. Alzheimers Dement. 2011;7 (1):e1–12. - PubMed
-
- Walsh DM, Klyubin I, Fadeeva JV, et al. Naturally secreted oligomers of amyloid beta protein potently inhibit hippocampal long-term potentiation in vivo. Nature. 2002;416 (6880):535–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
