

Rapid reduction in donor-specific anti-human leukocyte antigen antibodies and reversal of antibody-mediated rejection with bortezomib in pediatric heart transplant patients
- PMID: 22179403
- PMCID: PMC3730122
- DOI: 10.1097/TP.0b013e31823f7eea
Rapid reduction in donor-specific anti-human leukocyte antigen antibodies and reversal of antibody-mediated rejection with bortezomib in pediatric heart transplant patients
Abstract
Background: High titer donor-specific antibodies (DSA) and positive crossmatch in cardiac transplant recipients is associated with increased mortality from antibody-mediated rejection (AMR). Although treatment to reduce anti-human leukocyte antigen antibodies using plasmapheresis, intravenous immunoglobulin, and rituximab has been reported to be beneficial, in practice these are often ineffective. Moreover, these interventions do not affect the mature antibody producing plasma cell. Bortezomib, a proteasome inhibitor active against plasma cells, has been shown to reduce DSA in renal transplant patients with AMR. We report here the first use of bortezomib for cardiac transplant recipients in four pediatric heart recipients with biopsy-proven AMR, hemodynamic compromise, positive crossmatch, and high titer class I DSA.
Methods: Patients received four intravenous dose of bortezomib (1.3 mg/m(2)) over 2 weeks with plasmapheresis and rituximab. DSA specificity and strength (mean fluorescence intensity) was determined with Luminex. All had received previous treatment with plasmapheresis, intravenous immunoglobulin, and rituximab that was ineffective.
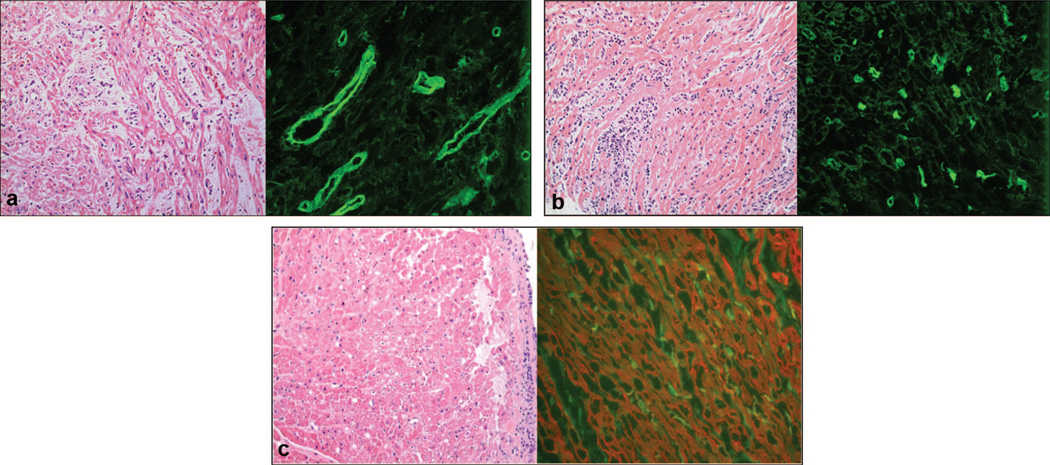
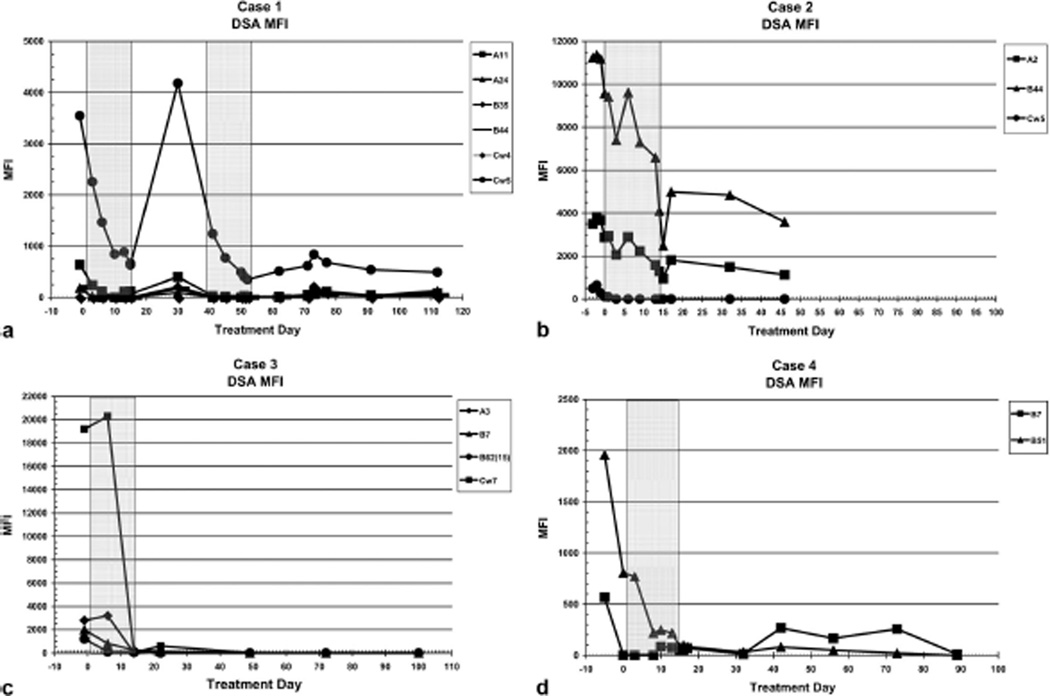
Results: AMR resolved in all patients treated with bortezomib with improvement in systolic function, conversion of biopsy to C4d negative in three patients and IgG negative in one patient, and a prompt, precipitous reduction in DSAs. In three patients who received plasmapheresis before bortezomib, plasmapheresis failed to reduce DSA. In one case, DSA increased after bortezomib but decreased after retreatment.
Conclusions: Bortezomib reduces DSA and may be an important adjunct to treatment of AMR in cardiac transplant recipients. Bortezomib may also be useful in desensitization protocols and in prevention of AMR in sensitized patients with positive crossmatch and elevated DSA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Proteasome inhibitor-based primary therapy for antibody-mediated renal allograft rejection.Transplantation. 2010 Feb 15;89(3):277-84. doi: 10.1097/TP.0b013e3181c6ff8d. Transplantation. 2010. PMID: 20145517
-
Lung transplantation across donor-specific anti-human leukocyte antigen antibodies: utility of bortezomib therapy in early graft dysfunction.Ann Pharmacother. 2012 Jan;46(1):e2. doi: 10.1345/aph.1Q509. Epub 2011 Dec 27. Ann Pharmacother. 2012. PMID: 22202499
-
Treatment of Biopsy-Proven Acute Antibody-Mediated Rejection Using Thymoglobulin (ATG) Monotherapy and a Combination of Rituximab, Intravenous Immunoglobulin, and Plasmapheresis: Lesson Learned from Primary Experience.Clin Transpl. 2014:223-30. Clin Transpl. 2014. PMID: 26281149
-
Proteasome inhibition with bortezomib: an effective therapy for severe antibody mediated rejection after renal transplantation.Clin Nephrol. 2012 Mar;77(3):246-53. doi: 10.5414/cn107156. Clin Nephrol. 2012. PMID: 22377258 Review.
-
Review of bortezomib treatment of antibody-mediated rejection in renal transplantation.Antioxid Redox Signal. 2014 Dec 10;21(17):2401-18. doi: 10.1089/ars.2014.5892. Epub 2014 Apr 28. Antioxid Redox Signal. 2014. PMID: 24635140 Review.
Cited by
-
Pediatric heart transplantation-indications and outcomes in the current era.J Thorac Dis. 2014 Aug;6(8):1080-96. doi: 10.3978/j.issn.2072-1439.2014.06.16. J Thorac Dis. 2014. PMID: 25132975 Free PMC article. Review.
-
The importance of non-HLA antibodies in transplantation.Nat Rev Nephrol. 2016 Aug;12(8):484-95. doi: 10.1038/nrneph.2016.88. Epub 2016 Jun 27. Nat Rev Nephrol. 2016. PMID: 27345243 Free PMC article. Review.
-
Reversing endogenous alloreactive B cell GC responses with anti-CD154 or CTLA-4Ig.Am J Transplant. 2013 Sep;13(9):2280-92. doi: 10.1111/ajt.12350. Epub 2013 Jul 15. Am J Transplant. 2013. PMID: 23855587 Free PMC article.
-
Interferon Gamma and Contact-dependent Cytotoxicity Are Each Rate Limiting for Natural Killer Cell-Mediated Antibody-dependent Chronic Rejection.Am J Transplant. 2016 Nov;16(11):3121-3130. doi: 10.1111/ajt.13865. Epub 2016 Jul 7. Am J Transplant. 2016. PMID: 27163757 Free PMC article.
-
Management of the sensitized pediatric heart transplant patient.Transl Pediatr. 2019 Oct;8(4):302-313. doi: 10.21037/tp.2019.07.13. Transl Pediatr. 2019. PMID: 31728323 Free PMC article. Review.
References
-
- Rose EA, Smith CR, Petrossian GA, et al. Humoral immune responses after cardiac transplantation: Correlation with fatal rejection and graft atherosclerosis. Surgery. 1989;106:203. - PubMed
-
- Lavee J, Kormos RL, Duquesnoy RJ, et al. Influence of panel-reactive antibody and lymphocytoxic crossmatch on survival after heart transplantation. J Heart Lung Transplant. 1991;10:921. - PubMed
-
- Smith JD, Danskine AJ, Laylor RM, et al. The effect of panel reactive antibodies and the donor specific crossmatch on graft survival after heart and heart-lung transplantation. Transplant Immunol. 1993;1:60. - PubMed
-
- Wright EJ, Fiser WP, Edens E, et al. Cardiac transplant outcomes in pediatric patients with pre-formed anti-human leukocyte antigen antibodies and/or positive retrospective crossmatch. J Heart Lung Transplant. 2007;26:1163. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
