

Improved survival time trends for glioblastoma using the SEER 17 population-based registries
- PMID: 21984115
- PMCID: PMC4077033
- DOI: 10.1007/s11060-011-0738-7
Improved survival time trends for glioblastoma using the SEER 17 population-based registries
Abstract
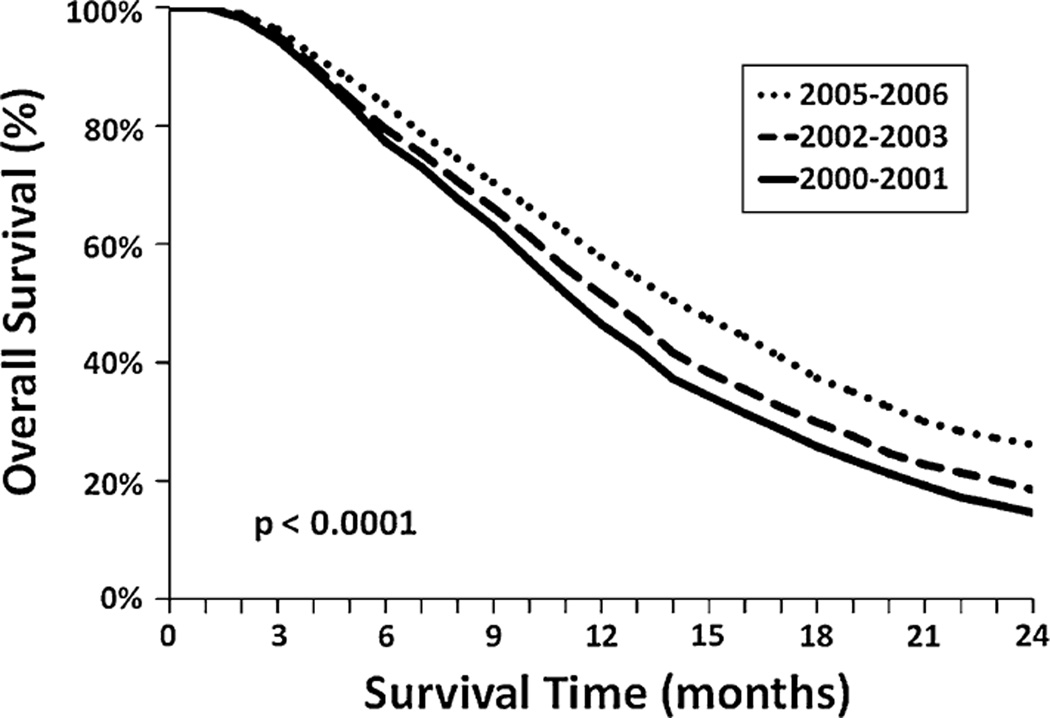
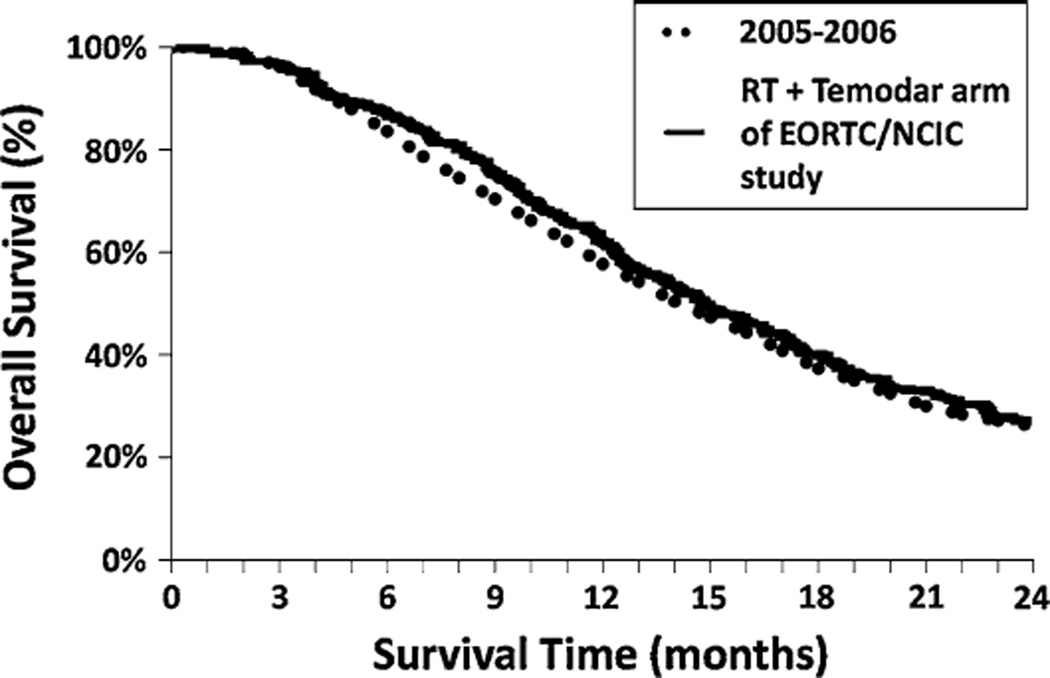
The EORTC/NCIC 22981/26981 study demonstrated an improvement in median overall survival (OS) from 12.1 to 14.6 months in patients with glioblastoma (GBM) who received temozolomide with post-operative radiotherapy (RT). The current study was performed to determine if those results translated into a survival benefit in a population-based cohort. Patients diagnosed between 2000 and 2006 with a GBM who underwent surgery and post-operative RT were selected from the Surveillance, Epidemiology and End Results database. Patients were grouped into time periods: 2000-2001, 2002-2003, 2004 and 2005-2006 (which represented those treated after the EORTC/NCIC trial presentation in 2004). Relative survival (RS) was estimated by the Kaplan-Meier method, and Cox multivariable regression modeling was used to estimate proportional hazard ratios (HR). Over time, there was improvement in the median and 2-year RS of 12 months and 15% for 2000-2001, 13 months and 19% for 2002-2003, 14 months and 24% for 2004, and 15 months and 26% for 2005-2006 (P < 0.0001 compared to 2000-2001 and 2002-2003; P = 0.07 compared to 2004). The estimated adjusted HR showed that patients diagnosed in 2005-2006 had significantly improved survival when compared to patients diagnosed in 2000-2001 (HR = 0.648, 95% CI 0.604-0.696). The median and 2 year RS of 15 months and 26% in 2005-2006 was similar to the median and 2 year OS of 14.6 months and 26% seen in the EORTC/NCIC phase III study. These results are encouraging and suggest that the current treatment of glioblastoma nationwide is now associated with an improved survival compared to previous time cohorts.
Conflict of interest statement
Figures
Similar articles
-
Clinical features associated with the efficacy of chemotherapy in patients with glioblastoma (GBM): a surveillance, epidemiology, and end results (SEER) analysis.BMC Cancer. 2021 Jan 19;21(1):81. doi: 10.1186/s12885-021-07800-0. BMC Cancer. 2021. PMID: 33468109 Free PMC article.
-
Survival benefit of glioblastoma patients after FDA approval of temozolomide concomitant with radiation and bevacizumab: A population-based study.Oncotarget. 2017 Jul 4;8(27):44015-44031. doi: 10.18632/oncotarget.17054. Oncotarget. 2017. PMID: 28467795 Free PMC article.
-
Survival of patients with newly diagnosed glioblastoma treated with radiation and temozolomide in research studies in the United States.Clin Cancer Res. 2010 Apr 15;16(8):2443-9. doi: 10.1158/1078-0432.CCR-09-3106. Epub 2010 Apr 6. Clin Cancer Res. 2010. PMID: 20371685 Free PMC article.
-
Gliadel wafer implantation combined with standard radiotherapy and concurrent followed by adjuvant temozolomide for treatment of newly diagnosed high-grade glioma: a systematic literature review.World J Surg Oncol. 2016 Aug 24;14(1):225. doi: 10.1186/s12957-016-0975-5. World J Surg Oncol. 2016. PMID: 27557526 Free PMC article. Review.
-
Glioblastoma: Part I. Current state of affairs.Mo Med. 2011 May-Jun;108(3):187-94. Mo Med. 2011. PMID: 21736079 Free PMC article. Review.
Cited by
-
The global immune-nutrition-inflammation index (GINI) as a robust prognostic factor in glioblastoma patients treated with the standard stupp protocol.Int J Immunopathol Pharmacol. 2024 Jan-Dec;38:3946320241284089. doi: 10.1177/03946320241284089. Int J Immunopathol Pharmacol. 2024. PMID: 39305006 Free PMC article.
-
Dissecting and rebuilding the glioblastoma microenvironment with engineered materials.Nat Rev Mater. 2019 Oct;4(10):651-668. doi: 10.1038/s41578-019-0135-y. Epub 2019 Aug 16. Nat Rev Mater. 2019. PMID: 32647587 Free PMC article.
-
Population-based survival data for brain tumors in Korea.J Neurooncol. 2012 Sep;109(2):301-7. doi: 10.1007/s11060-012-0893-5. Epub 2012 Jun 4. J Neurooncol. 2012. PMID: 22660961
-
Analysis of IDH and EGFR as biomarkers in glioblastoma multiforme: A case-control study.Heliyon. 2024 Jul 26;10(15):e35323. doi: 10.1016/j.heliyon.2024.e35323. eCollection 2024 Aug 15. Heliyon. 2024. PMID: 39165999 Free PMC article.
-
Reduction of Human Glioblastoma Spheroids Using Cold Atmospheric Plasma: The Combined Effect of Short- and Long-Lived Reactive Species.Cancers (Basel). 2018 Oct 23;10(11):394. doi: 10.3390/cancers10110394. Cancers (Basel). 2018. PMID: 30360539 Free PMC article.
References
-
- Tran B, Rosenthal MA. Survival comparison between glioblastoma multiforme and other incurable cancers. J Clin Neurosci. 2010;17:417–421. - PubMed
-
- Buckner JC. Factors influencing survival in high-grade gliomas. Semin Oncol. 2003;30:10–14. - PubMed
-
- Curran WJ, Jr, Scott CB, Horton J, Nelson JS, Weinstein AS, Fischbach AJ, Chang CH, Rotman M, Asbell SO, Krisch RE. Recursive partitioning analysis of prognostic factors in three Radiation Therapy Oncology Group malignant glioma trials. J Natl Cancer Inst. 1993;85:704–710. - PubMed
-
- DeAngelis LM. Brain tumors. N Engl J Med. 2001;344:114–123. - PubMed
-
- CBTRUS. CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2004–2007. 2010
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
