

Decreased lymphangiogenesis and lymph node metastasis by mTOR inhibition in head and neck cancer
- PMID: 21975930
- PMCID: PMC3443559
- DOI: 10.1158/0008-5472.CAN-10-3192
Decreased lymphangiogenesis and lymph node metastasis by mTOR inhibition in head and neck cancer
Erratum in
- Cancer Res. 2012 Feb 1;72(3):826. Nathan, Cherie Ann [corrected to Nathan, Cherie-Ann O]
Abstract
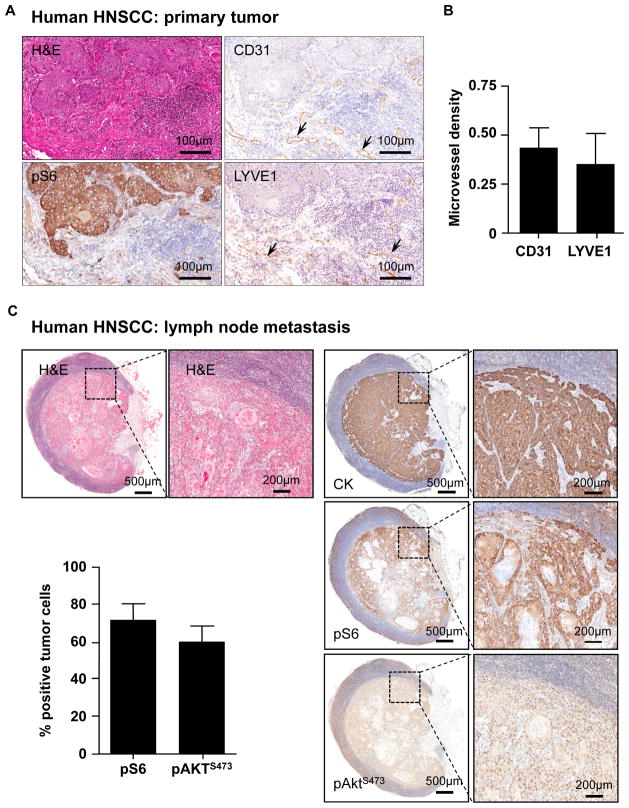
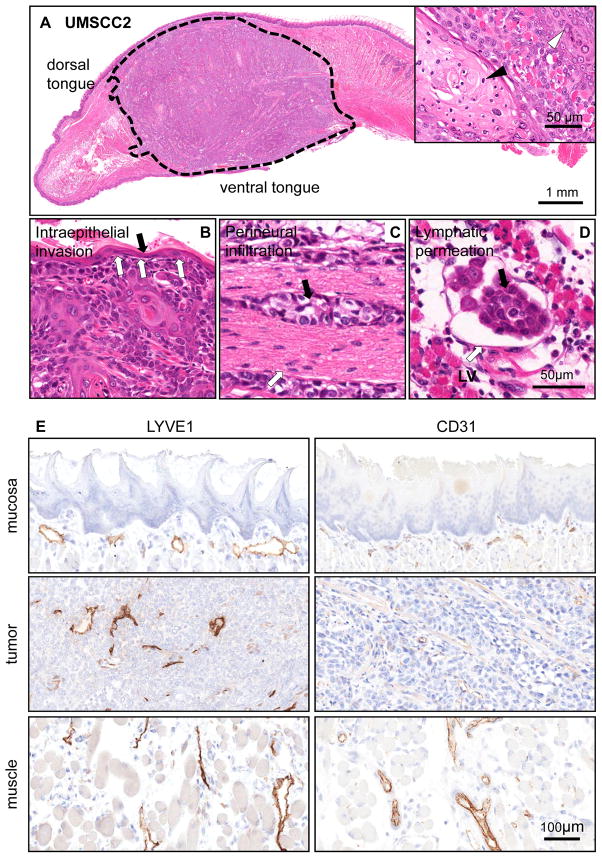
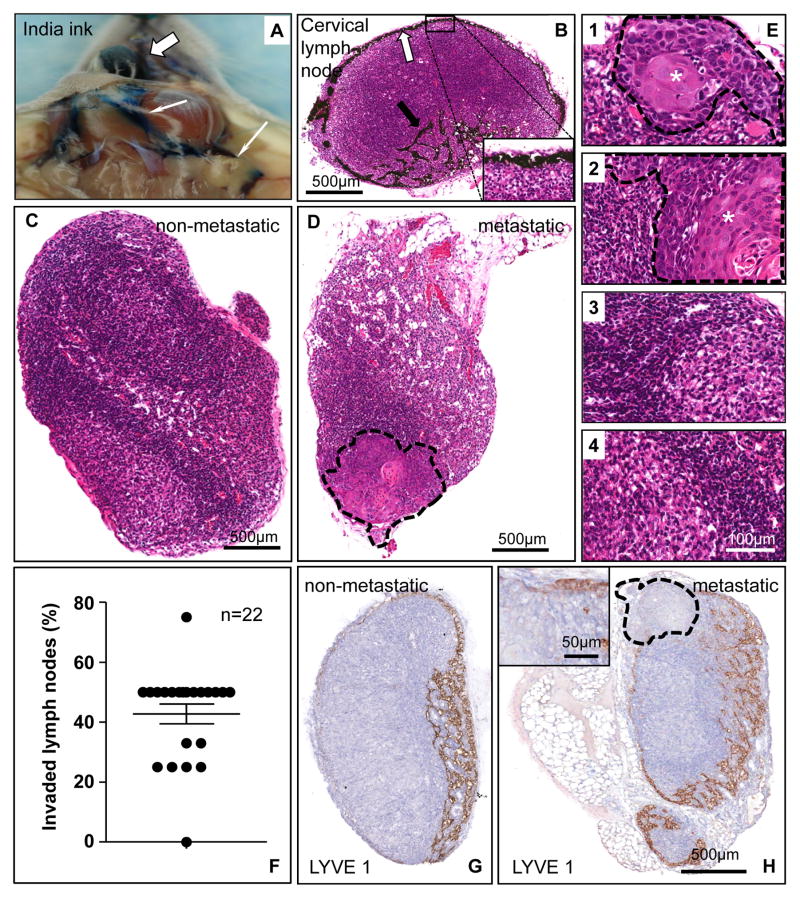
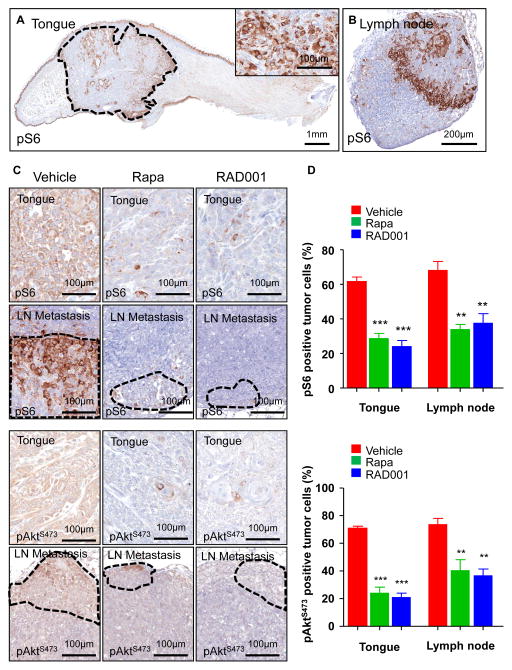
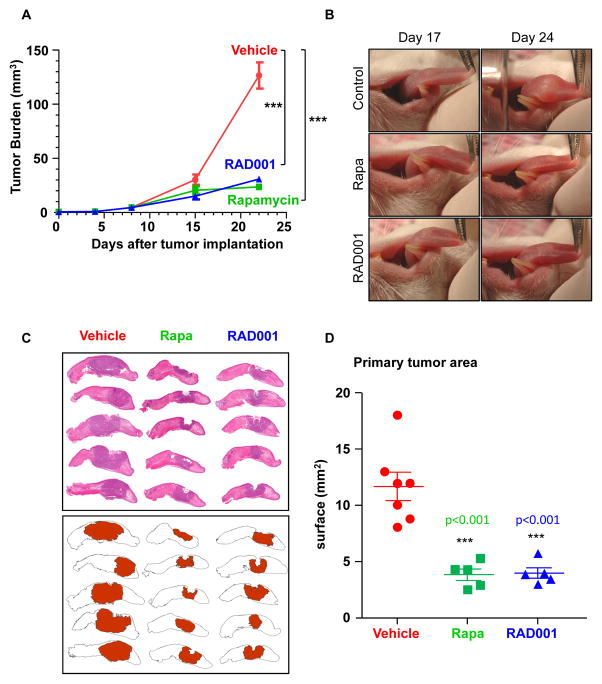
Despite our improved understanding of cancer, the 5-year survival rate for head and neck squamous cell carcinomas (HNSCC) patients remains relatively unchanged at 50% for the past three decades. HNSCCs often metastasize to locoregional lymph nodes, and lymph node involvement represents one of the most important prognostic factors of poor clinical outcome. Among the multiple dysregulated molecular mechanism in HNSCCs, emerging basic, preclinical, and clinical findings support the importance of the mTOR signaling route in HNSCC progression. Indeed, we observed here that the activation of mTOR is a widespread event in clinical specimens of HNSCCs invading locoregional lymph nodes. We developed an orthotopic model of HNSCC consisting of the implantation of HNSCC cells into the tongues of immunocompromised mice. These orthotopic tumors spontaneously metastasize to the cervical lymph nodes, where the presence of HNSCC cells can be revealed by histologic and immunohistochemical evaluation. Both primary and metastatic experimental HNSCC lesions exhibited elevated mTOR activity. The ability to monitor and quantitate lymph node invasion in this model system enabled us to explore whether the blockade of mTOR could impact HNSCC metastasis. We found that inhibition of mTOR with rapamycin and the rapalog RAD001 diminished lymphangiogenesis in the primary tumors and prevented the dissemination of HNSCC cancer cells to the cervical lymph nodes, thereby prolonging animal survival. These findings may provide a rationale for the future clinical evaluation of mTOR inhibitors, including rapamycin and its analogues, as part of a molecular-targeted metastasis preventive strategy for the treatment of patients with HNSCC.
©2011 AACR
Conflict of interest statement
Figures

Similar articles
-
Anti-lymphangiogenic properties of mTOR inhibitors in head and neck squamous cell carcinoma experimental models.BMC Cancer. 2013 Jul 1;13:320. doi: 10.1186/1471-2407-13-320. BMC Cancer. 2013. PMID: 23815869 Free PMC article.
-
Genetic Identification of SEMA3F as an Antilymphangiogenic Metastasis Suppressor Gene in Head and Neck Squamous Carcinoma.Cancer Res. 2015 Jul 15;75(14):2937-48. doi: 10.1158/0008-5472.CAN-14-3121. Epub 2015 May 7. Cancer Res. 2015. PMID: 25952650 Free PMC article.
-
mTOR as a molecular target in HPV-associated oral and cervical squamous carcinomas.Clin Cancer Res. 2012 May 1;18(9):2558-68. doi: 10.1158/1078-0432.CCR-11-2824. Epub 2012 Mar 12. Clin Cancer Res. 2012. PMID: 22409888 Free PMC article.
-
mTOR inhibitors and its role in the treatment of head and neck squamous cell carcinoma.Curr Treat Options Oncol. 2012 Mar;13(1):71-81. doi: 10.1007/s11864-011-0180-2. Curr Treat Options Oncol. 2012. PMID: 22282394 Review.
-
Mammalian target of rapamycin and head and neck squamous cell carcinoma.Head Neck Oncol. 2011 Apr 24;3:22. doi: 10.1186/1758-3284-3-22. Head Neck Oncol. 2011. PMID: 21513566 Free PMC article. Review.
Cited by
-
Metformin prevents the development of oral squamous cell carcinomas from carcinogen-induced premalignant lesions.Cancer Prev Res (Phila). 2012 Apr;5(4):562-73. doi: 10.1158/1940-6207.CAPR-11-0502. Epub 2012 Mar 31. Cancer Prev Res (Phila). 2012. PMID: 22467081 Free PMC article.
-
An in vivo method to quantify lymphangiogenesis in zebrafish.PLoS One. 2012;7(9):e45240. doi: 10.1371/journal.pone.0045240. Epub 2012 Sep 13. PLoS One. 2012. PMID: 23028871 Free PMC article.
-
Application of microscale culture technologies for studying lymphatic vessel biology.Microcirculation. 2019 Nov;26(8):e12547. doi: 10.1111/micc.12547. Epub 2019 May 2. Microcirculation. 2019. PMID: 30946511 Free PMC article. Review.
-
A multicenter study on expressions of vascular endothelial growth factor, matrix metallopeptidase-9 and tissue inhibitor of metalloproteinase-2 in oral and maxillofacial squamous cell carcinoma.Iran Red Crescent Med J. 2014 Mar;16(3):e13185. doi: 10.5812/ircmj.13185. Epub 2014 Mar 5. Iran Red Crescent Med J. 2014. PMID: 24829764 Free PMC article.
-
Suppression of the Growth and Invasion of Human Head and Neck Squamous Cell Carcinomas via Regulating STAT3 Signaling and the miR-21/β-catenin Axis with HJC0152.Mol Cancer Ther. 2017 Apr;16(4):578-590. doi: 10.1158/1535-7163.MCT-16-0606. Epub 2017 Jan 30. Mol Cancer Ther. 2017. PMID: 28138036 Free PMC article.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–49. - PubMed
-
- Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009;45:309–16. - PubMed
-
- Haddad RI, Shin DM. Recent advances in head and neck cancer. N Engl J Med. 2008;359:1143–54. - PubMed
-
- Forastiere A, Koch W, Trotti A, Sidransky D. Head and neck cancer. N Engl J Med. 2001;345:1890–900. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
