

Asymptomatic primary Merkel cell polyomavirus infection among adults
- PMID: 21801612
- PMCID: PMC3381535
- DOI: 10.3201/eid1708.110079
Asymptomatic primary Merkel cell polyomavirus infection among adults
Abstract
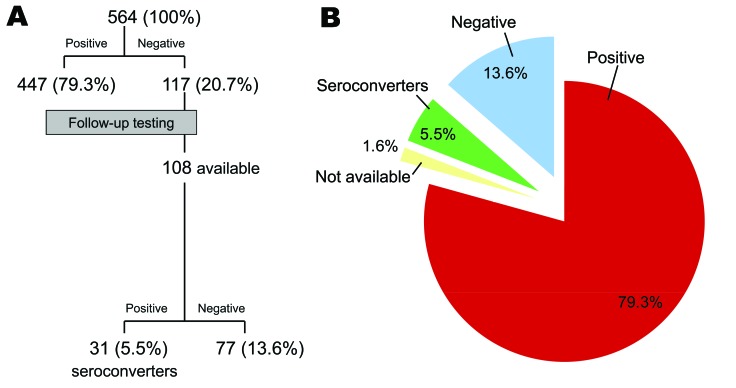
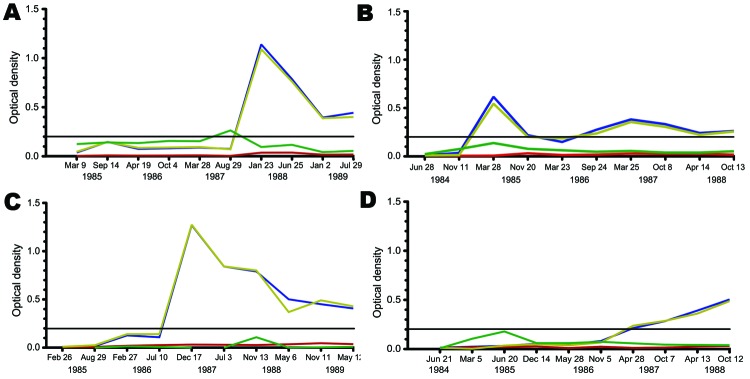
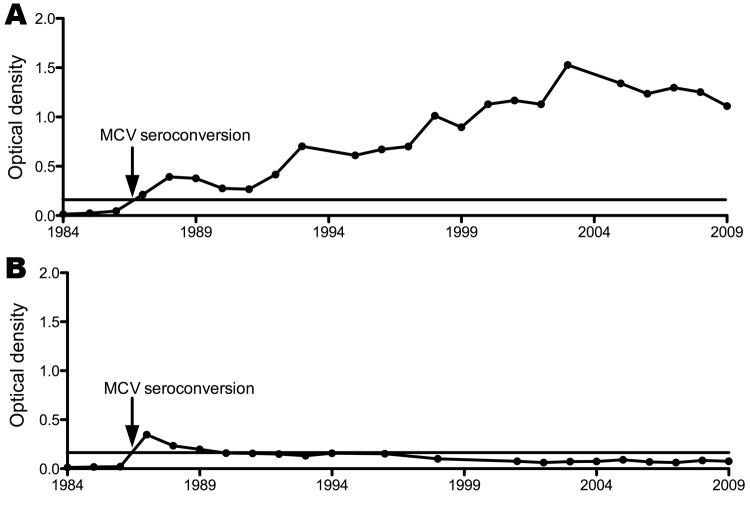
Merkel cell polyomavirus (MCV) is a recently discovered virus that causes 80% of Merkel cell carcinomas. We examined data for 564 gay/bisexual male participants >18 years of age in the Multicenter AIDS Cohort Study in Pittsburgh, Pennsylvania, USA, and found that 447 (79.3%) were MCV-antibody positive at initial enrollment. Of the 117 MCV-seronegative men, 31 subsequently seroconverted over a 4-year follow-up period, corresponding to a 6.6% annual conversion rate. MCV immunoglobulin G levels remained detectable up to 25 years after exposure. No signs, symptoms, or routine diagnostic test results were associated with MCV infection, and no correlation between HIV infection or AIDS progression and MCV infection was noted. An initial correlation between chronic hepatitis B virus infection and MCV prevalence could not be confirmed among MCV seroconverters or in studies of a second hepatitis B virus-hyperendemic cohort from Qidong, China. In adults, MCV is typically an asymptomatic, common, and commensal viral infection that initiates rare cancers after virus (rather than host cell) mutations.
Figures

Similar articles
-
Prospective study of Merkel cell polyomavirus and risk of Merkel cell carcinoma.Int J Cancer. 2014 Feb 15;134(4):844-8. doi: 10.1002/ijc.28419. Epub 2013 Aug 29. Int J Cancer. 2014. PMID: 23922031
-
The Merkel cell polyomavirus and its involvement in Merkel cell carcinoma.Dermatol Surg. 2013 Feb;39(2):232-8. doi: 10.1111/dsu.12079. Dermatol Surg. 2013. PMID: 23387356 Review.
-
Prognostication in Merkel cell carcinoma.Expert Rev Anticancer Ther. 2011 May;11(5):665-7. doi: 10.1586/era.11.50. Expert Rev Anticancer Ther. 2011. PMID: 21554038 No abstract available.
-
Epidemiological, Clinicopathological and Virological Features of Merkel Cell Carcinomas in Medical Center of University of Pécs, Hungary (2007-2012).Pathol Oncol Res. 2016 Jan;22(1):71-7. doi: 10.1007/s12253-015-9974-z. Epub 2015 Aug 26. Pathol Oncol Res. 2016. PMID: 26306468
-
Merkel cell carcinoma: a virus-induced human cancer.Annu Rev Pathol. 2012;7:123-44. doi: 10.1146/annurev-pathol-011110-130227. Epub 2011 Sep 13. Annu Rev Pathol. 2012. PMID: 21942528 Free PMC article. Review.
Cited by
-
Merkel cell carcinoma of the abdominal wall.Indian Dermatol Online J. 2015 Jul-Aug;6(4):269-73. doi: 10.4103/2229-5178.160262. Indian Dermatol Online J. 2015. PMID: 26225333 Free PMC article.
-
A cornucopia of human polyomaviruses.Nat Rev Microbiol. 2013 Apr;11(4):264-76. doi: 10.1038/nrmicro2992. Epub 2013 Mar 11. Nat Rev Microbiol. 2013. PMID: 23474680 Free PMC article. Review.
-
Decreased IgG Antibody Response to Viral Protein Mimotopes of Oncogenic Merkel Cell Polyomavirus in Sera From Healthy Elderly Subjects.Front Immunol. 2021 Oct 18;12:738486. doi: 10.3389/fimmu.2021.738486. eCollection 2021. Front Immunol. 2021. PMID: 34733278 Free PMC article.
-
Cellular and viral factors regulating Merkel cell polyomavirus replication.PLoS One. 2011;6(7):e22468. doi: 10.1371/journal.pone.0022468. Epub 2011 Jul 22. PLoS One. 2011. PMID: 21799863 Free PMC article.
-
A Novel In Vitro Culture Model System to Study Merkel Cell Polyomavirus-Associated MCC Using Three-Dimensional Organotypic Raft Equivalents of Human Skin.Viruses. 2021 Jan 19;13(1):138. doi: 10.3390/v13010138. Viruses. 2021. PMID: 33478104 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical