

Integrative analysis of type-I and type-II aberrations underscores the genetic heterogeneity of pediatric acute myeloid leukemia
- PMID: 21791472
- PMCID: PMC3186309
- DOI: 10.3324/haematol.2010.038976
Integrative analysis of type-I and type-II aberrations underscores the genetic heterogeneity of pediatric acute myeloid leukemia
Abstract
Background: Several studies of pediatric acute myeloid leukemia have described the various type-I or type-II aberrations and their relationship with clinical outcome. However, there has been no recent comprehensive overview of these genetic aberrations in one large pediatric acute myeloid leukemia cohort.
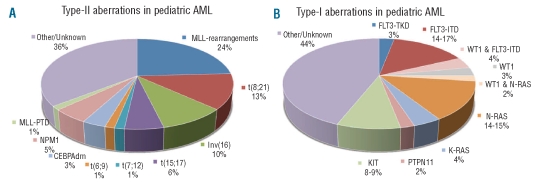
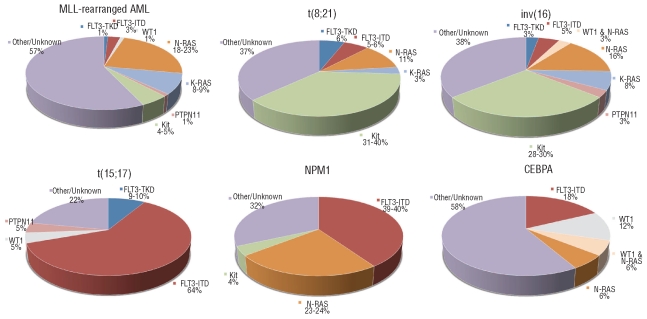
Design and methods: We studied the different genetic aberrations, their associations and their impact on prognosis in a large pediatric acute myeloid leukemia series (n=506). Karyotypes were studied, and hotspot regions of NPM1, CEPBA, MLL, WT1, FLT3, N-RAS, K-RAS, PTPN11 and KIT were screened for mutations of available samples. The mutational status of all type-I and type-II aberrations was available in 330 and 263 cases, respectively. Survival analysis was performed in a subset (n=385) treated on consecutive acute myeloid leukemia Berlin-Frankfurt-Munster Study Group and Dutch Childhood Oncology Group treatment protocols.
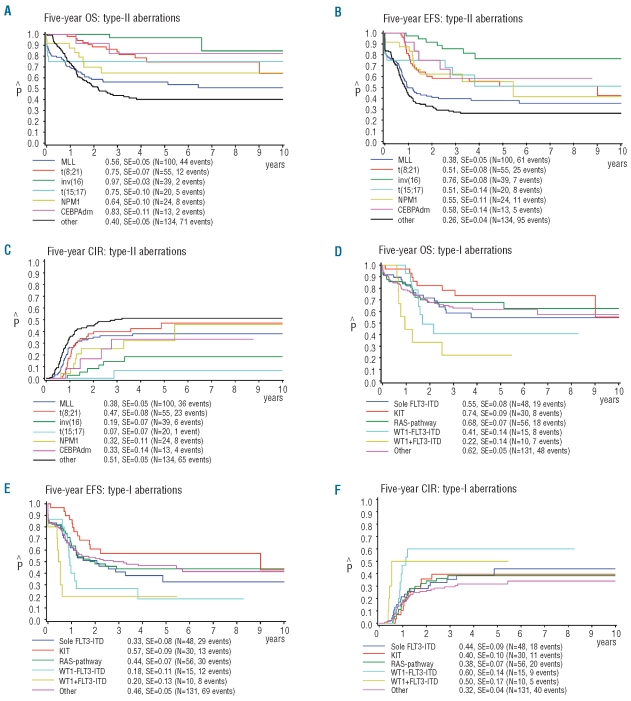
Results: Genetic aberrations were associated with specific clinical characteristics, e.g. significantly higher diagnostic white blood cell counts in MLL-rearranged, WT1-mutated and FLT3-ITD-positive acute myeloid leukemia. Furthermore, there was a significant difference in the distribution of these aberrations between children below and above the age of two years. Non-random associations, e.g. KIT mutations with core-binding factor acute myeloid leukemia, and FLT3-ITD with t(15;17)(q22;q21), NPM1- and WT1-mutated acute myeloid leukemia, respectively, were observed. Multivariate analysis revealed a 'favorable karyotype', i.e. t(15;17)(q22;q21), t(8;21)(q22;q22) and inv(16)(p13q22)/t(16;16)(p13;q22). NPM1 and CEBPA double mutations were independent factors for favorable event-free survival. WT1 mutations combined with FLT3-ITD showed the worst outcome for 5-year overall survival (22±14%) and 5-year event-free survival (20±13%), although it was not an independent factor in multivariate analysis.
Conclusions: Integrative analysis of type-I and type-II aberrations provides an insight into the frequencies, non-random associations and prognostic impact of the various aberrations, reflecting the heterogeneity of pediatric acute myeloid leukemia. These aberrations are likely to guide the stratification of pediatric acute myeloid leukemia and may direct the development of targeted therapies.
Figures
Similar articles
-
Evaluation of gene expression signatures predictive of cytogenetic and molecular subtypes of pediatric acute myeloid leukemia.Haematologica. 2011 Feb;96(2):221-30. doi: 10.3324/haematol.2010.029660. Epub 2010 Oct 22. Haematologica. 2011. PMID: 20971820 Free PMC article.
-
High WT1 mRNA expression after induction chemotherapy and FLT3-ITD have prognostic impact in pediatric acute myeloid leukemia: a study of the Japanese Childhood AML Cooperative Study Group.Int J Hematol. 2012 Oct;96(4):469-76. doi: 10.1007/s12185-012-1163-1. Epub 2012 Aug 23. Int J Hematol. 2012. PMID: 22915059
-
Prognostic significance of CEBPA mutations in a large cohort of younger adult patients with acute myeloid leukemia: impact of double CEBPA mutations and the interaction with FLT3 and NPM1 mutations.J Clin Oncol. 2010 Jun 1;28(16):2739-47. doi: 10.1200/JCO.2009.26.2501. Epub 2010 May 3. J Clin Oncol. 2010. PMID: 20439648
-
Prognostic significance of FLT3 internal tandem duplication, nucleophosmin 1, and CEBPA gene mutations for acute myeloid leukemia patients with normal karyotype and younger than 60 years: a systematic review and meta-analysis.Ann Hematol. 2014 Aug;93(8):1279-86. doi: 10.1007/s00277-014-2072-6. Epub 2014 May 7. Ann Hematol. 2014. PMID: 24801015 Review.
-
Cytogenetic, molecular genetic, and clinical characteristics of acute myeloid leukemia with a complex karyotype.Semin Oncol. 2008 Aug;35(4):365-77. doi: 10.1053/j.seminoncol.2008.04.007. Semin Oncol. 2008. PMID: 18692687 Free PMC article. Review.
Cited by
-
HOXA11 plays critical roles in disease progression and response to cytarabine in AML.Oncol Rep. 2021 Jul;46(1):150. doi: 10.3892/or.2021.8101. Epub 2021 Jun 3. Oncol Rep. 2021. PMID: 34080665 Free PMC article.
-
Telomere length and telomerase complex mutations in pediatric acute myeloid leukemia.Leukemia. 2013 Aug;27(8):1786-9. doi: 10.1038/leu.2013.57. Epub 2013 Feb 21. Leukemia. 2013. PMID: 23426163 Free PMC article. No abstract available.
-
Straight to the Point-The Novel Strategies to Cure Pediatric AML.Int J Mol Sci. 2022 Feb 10;23(4):1968. doi: 10.3390/ijms23041968. Int J Mol Sci. 2022. PMID: 35216084 Free PMC article. Review.
-
First mouse model of infant acute myeloid leukemia with t(7;12)(q36;p17).Haematologica. 2024 Mar 1;109(3):712-714. doi: 10.3324/haematol.2023.283659. Haematologica. 2024. PMID: 37584296 Free PMC article. No abstract available.
-
Prognostic Significance of NRAS Gene Mutations in Children with Acute Myelogenous Leukemia.Mediterr J Hematol Infect Dis. 2011;3(1):e2011055. doi: 10.4084/MJHID.2011.055. Epub 2011 Nov 28. Mediterr J Hematol Infect Dis. 2011. PMID: 22220252 Free PMC article.
References
-
- Downing JR, Shannon KM. Acute leukemia: a pediatric perspective. Cancer Cell. 2002;2(6):437–45. - PubMed
-
- Kaspers GJ, Zwaan CM. Pediatric acute myeloid leukemia: towards high-quality cure of all patients. Haematologica. 2007;92(11):1519–32. - PubMed
-
- Raimondi SC, Chang MN, Ravindranath Y, Behm FG, Gresik MV, Steuber CP, et al. Chromosomal abnormalities in 478 children with acute myeloid leukemia: clinical characteristics and treatment outcome in a cooperative pediatric oncology group study-POG 8821. Blood. 1999;94(11):3707–16. - PubMed
-
- Harrison CJ, Hills RK, Moorman AV, Grimwade DJ, Hann I, Webb DK, et al. Cytogenetics of childhood acute myeloid leukemia: United Kingdom Medical Research Council. Treatment trials AML 10 and 12. J Clin Oncol. 28(16):2674–81. - PubMed
-
- von Neuhoff C, Reinhardt D, Sander A, Zimmermann M, Bradtke J, Betts DR, et al. Prognostic impact of specific chromosomal aberrations in a large group of pediatric patients with acute myeloid leukemia treated uniformly according to trial AML-BFM 98. J Clin Oncol. 2010;28(16):2682–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
