

Review
doi: 10.1186/bcr2890.
Microarrays in the 2010s: the contribution of microarray-based gene expression profiling to breast cancer classification, prognostication and prediction
Affiliations
- PMID: 21787441
- PMCID: PMC3218943
- DOI: 10.1186/bcr2890
Item in Clipboard
Review
Microarrays in the 2010s: the contribution of microarray-based gene expression profiling to breast cancer classification, prognostication and prediction
Breast Cancer Res.
.
Abstract
Breast cancer comprises a collection of diseases with distinctive clinical, histopathological, and molecular features. Importantly, tumors with similar histological features may display disparate clinical behaviors. Gene expression profiling using microarray technologies has improved our understanding of breast cancer biology and has led to the development of a breast cancer molecular taxonomy and of multigene 'signatures' to predict outcome and response to systemic therapies. The use of these prognostic and predictive signatures in routine clinical decision-making remains controversial. Here, we review the clinical relevance of microarray-based profiling of breast cancer and discuss its impact on patient management.
Figures
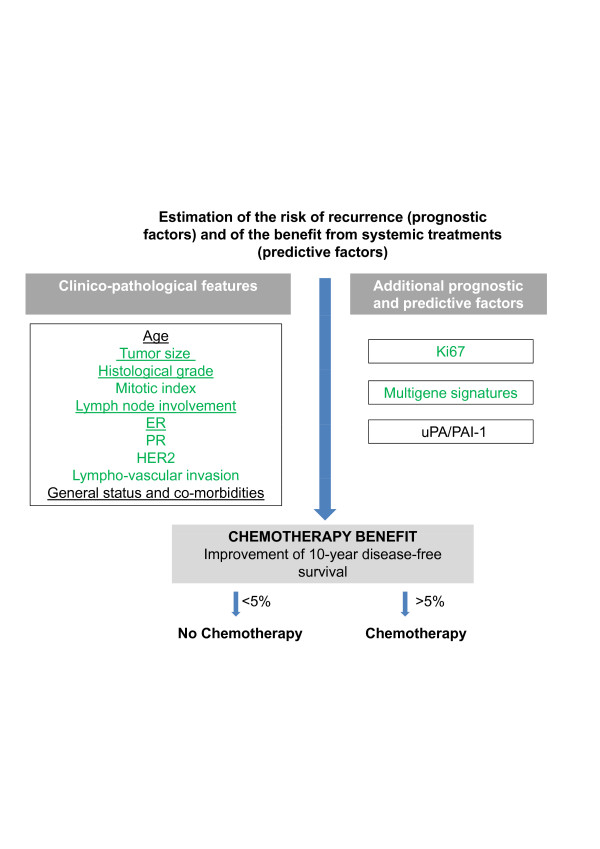
Clinical decision-making for adjuvant chemotherapy. Criteria included in the St. Gallen guidelines (green font) and in Adjuvant! Online (underlined) are shown. ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; uPA/PAI-1, urokinase-type plasminogen activator and plasminogen activator inhibitor-1.
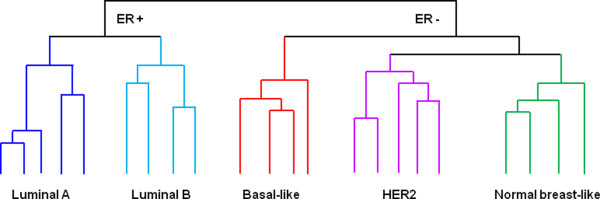
Schematic illustrations of the five major clusters that represent the molecular subtypes of breast cancer. Perou and colleagues [11] carried out a cDNA microarray analysis of 38 invasive breast cancers, 1 ductal carcinoma in situ, 1 fibroadenoma and 3 normal breast samples, and a number of biological replicates of tumors from the same patients and defined an 'intrinsic gene' list (that is, genes that vary more between tumors from different patients compared with samples from the same tumor/patient). Hierarchical clustering analysis using these 'intrinsic' genes led to the identification of four subtypes: luminal, normal breast-like, human epidermal growth factor receptor 2 (HER2), and basal-like. In subsequent studies, it was demonstrated that similar molecular subtypes of breast cancer could be identified in multiple cohorts and that luminal cancers could be subclassified into two groups (luminal A and B) [12] or three groups (luminal A, B, and C) [13]. The estrogen receptor (ER)-positive branch of the dendrogram contains the luminal tumors, which express low-molecular weight cytokeratins 8/18, ER, and genes associated with an active ER pathway [2,3,11-13,17,26,34]. Luminal A tumors (dark blue) present high levels of expression of ER-activated genes and low proliferation rates and are associated with an excellent prognosis, whereas luminal B breast cancers (light blue) are more often of higher histological grade and have higher proliferation rates and a worse prognosis [2,3,11-13,17,26,34]. The ER-negative branch includes at least three subtypes: normal breast-like, HER2, and basal-like. HER2 tumors (purple) overexpress HER2 and genes associated with the HER2 amplicon on 17q12 (that is, GRB7) and/or the HER2 pathway [2,3,11-13,17,26,34]. Basal-like tumors (red) express genes usually found in normal basal/myoepithelial cells of the breast, including high-molecular weight cytokeratins (5 and 17), caveolins 1 and 2, P-cadherin, nestin, CD44, and EGFR [20]. Morphological and immunohistochemical features of basal-like cancers are similar to those described for tumors arising in BRCA1 germ-line mutation carriers [20]. The HER2 and basal-like subgroups share an aggressive clinical behavior. Normal breast-like cancers (green) are still poorly characterized [3,22] and there is evidence to suggest that they may constitute an artefact of gene expression profiling associated with a disproportionately high content of normal breast tissue [3,17,26,34].
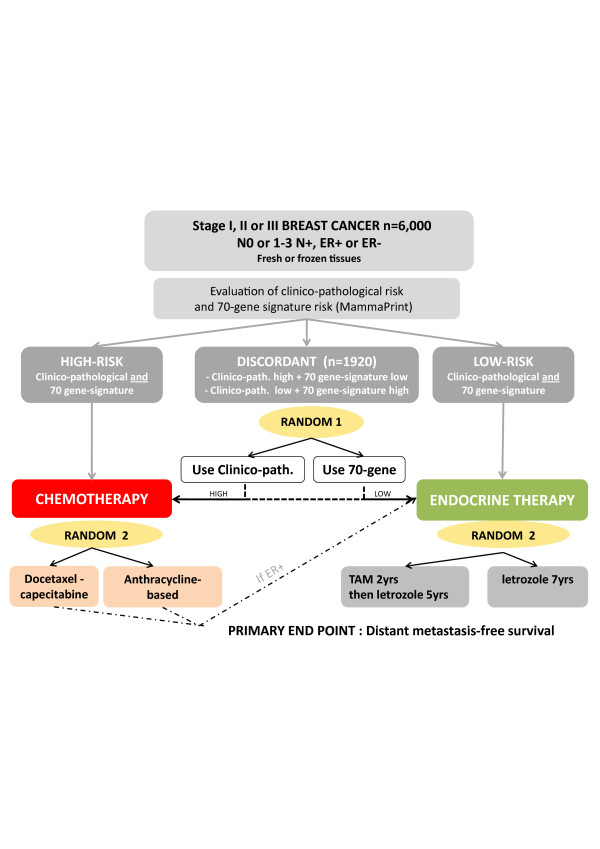
MINDACT (Microarray In Node-negative and 1-3 positive lymph-node Disease may Avoid ChemoTherapy) randomized trial design. The clinical impact of MammaPrint is being evaluated in MINDACT, a prospective multicenter randomized trial conducted by the European Organization for Research and Treatment of Cancer. The trial compares the recurrence-risk assessment of the 70-gene signature with that provided by Adjuvant! Online in selecting patients for adjuvant chemotherapy. Patients with concordant results are being treated accordingly (high-risk: chemotherapy with or without endocrine therapy, depending on estrogen receptor (ER) status; low-risk: hormonal therapy if ER-positive without chemotherapy). Discordant cases are being randomly assigned to receive adjuvant therapy on the basis of either clinicopathological or 70-gene signature risk assessment. Launched in 2006, the trial intends to confirm the validity of the signature and demonstrate that its clinical use would reduce the number of patients receiving unnecessary treatments, but the results will probably take years to be revealed. Clinico-path, clinicopathological; N, lymph node; N0, lymph node-negative; RANDOM, randomization; TAM, tamoxifen; yrs, years.
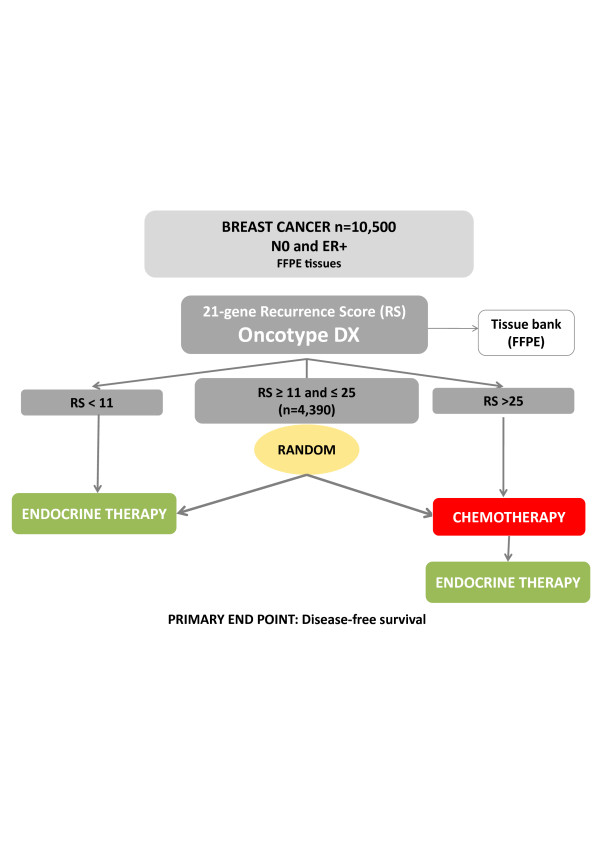
TAILORx (Trial Assigning IndividuaLized Options for Treatment Rx) randomized trial design. Oncotype DX is being tested in TAILORx, a prospective randomized phase III trial coordinated by the Breast Cancer Intergroup. The purposes of this trial are to confirm the prognostic value of the 21-gene recurrence score (RS), to determine the optimal management of patients with intermediate-RS, and to refine the utility of the assay in clinical practice. The accrual was recently completed and the first results will be disclosed in 2013. Patients with estrogen receptor (ER)-positive, node-negative breast cancers were eligible and were separated in three study groups according to their RS. High-RS patients (RS >25) received chemotherapy plus endocrine therapy, whereas low-RS patients (RS <11) were assigned to endocrine therapy alone. Patients with intermediate-RS (RS = 11 to 25) were randomly assigned to receive either hormonal therapy alone or hormonal therapy plus chemotherapy. To minimize potential under-treatment in both the high-risk and the randomly assigned groups, the RS ranges for TAILORx were different from those originally defined (11 to 25 instead of 18 to 31). FFPE, formalin-fixed paraffin-embedded; N0, lymph node-negative; RANDOM, randomization.
Similar articles
-
The contribution of gene expression profiling to breast cancer classification, prognostication and prediction: a retrospective of the last decade.J Pathol. 2010 Jan;220(2):263-80. doi: 10.1002/path.2648. J Pathol. 2010. PMID: 19927298 Review.
-
Microarray-based gene expression profiling as a clinical tool for breast cancer management: are we there yet?Int J Surg Pathol. 2009 Aug;17(4):285-302. doi: 10.1177/1066896908328577. Epub 2008 Dec 22. Int J Surg Pathol. 2009. PMID: 19103611 Review.
-
Microarray technology and its effect on breast cancer (re)classification and prediction of outcome.Breast Cancer Res. 2003;5(6):303-4. doi: 10.1186/bcr732. Epub 2003 Oct 9. Breast Cancer Res. 2003. PMID: 14580246 Free PMC article. No abstract available.
-
Discerning Clinical Responses in Breast Cancer Based On Molecular Signatures.Am J Pathol. 2017 Oct;187(10):2199-2207. doi: 10.1016/j.ajpath.2017.08.002. Epub 2017 Aug 16. Am J Pathol. 2017. PMID: 28822803 Review.
-
Histological types of breast cancer: how special are they?Mol Oncol. 2010 Jun;4(3):192-208. doi: 10.1016/j.molonc.2010.04.004. Epub 2010 Apr 18. Mol Oncol. 2010. PMID: 20452298 Free PMC article. Review.
Cited by
-
Are breast cancer molecular classes predictive of survival in patients with long follow-up?Dis Markers. 2013;35(6):595-605. doi: 10.1155/2013/347073. Epub 2013 Oct 30. Dis Markers. 2013. PMID: 24288429 Free PMC article.
-
MVIAeval: a web tool for comprehensively evaluating the performance of a new missing value imputation algorithm.BMC Bioinformatics. 2017 Jan 13;18(1):31. doi: 10.1186/s12859-016-1429-3. BMC Bioinformatics. 2017. PMID: 28086746 Free PMC article.
-
Targeting Intracellular Calcium Signaling ([Ca2+]i) to Overcome Acquired Multidrug Resistance of Cancer Cells: A Mini-Overview.Cancers (Basel). 2017 May 9;9(5):48. doi: 10.3390/cancers9050048. Cancers (Basel). 2017. PMID: 28486397 Free PMC article. Review.
-
Screening-relevant age threshold of 70 years and older is a stronger determinant for the choice of adjuvant treatment in breast cancer patients than tumor biology.Breast Cancer Res Treat. 2017 May;163(1):119-130. doi: 10.1007/s10549-017-4151-6. Epub 2017 Feb 15. Breast Cancer Res Treat. 2017. PMID: 28205042 Free PMC article.
-
Genomic instability at the 13q31 locus and somatic mtDNA mutation in the D-loop site correlate with tumor aggressiveness in sporadic Brazilian breast cancer cases.Clinics (Sao Paulo). 2012 Oct;67(10):1181-90. doi: 10.6061/clinics/2012(10)10. Clinics (Sao Paulo). 2012. PMID: 23070345 Free PMC article.
References
-
- Reis-Filho JS, Weigelt B, Fumagalli D, Sotiriou C. Molecular profiling: moving away from tumor philately. Sci Transl Med. 2010;2:47ps43. - PubMed
-
- Weigelt B, Baehner FL, Reis-Filho JS. The contribution of gene expression profiling to breast cancer classification, prognostication and prediction: a retrospective of the last decade. J Pathol. 2010;220:263–280. - PubMed
-
- Adjuvant! Online homepage. https://www.adjuvantonline.com
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
