

Phase I pharmacokinetic and pharmacodynamic study of the multikinase inhibitor sorafenib in combination with clofarabine and cytarabine in pediatric relapsed/refractory leukemia
- PMID: 21768474
- PMCID: PMC3158600
- DOI: 10.1200/JCO.2011.34.7427
Phase I pharmacokinetic and pharmacodynamic study of the multikinase inhibitor sorafenib in combination with clofarabine and cytarabine in pediatric relapsed/refractory leukemia
Abstract
Purpose: To assess the toxicity, pharmacokinetics, and pharmacodynamics of multikinase inhibitor sorafenib in combination with clofarabine and cytarabine in children with relapsed/refractory leukemia.
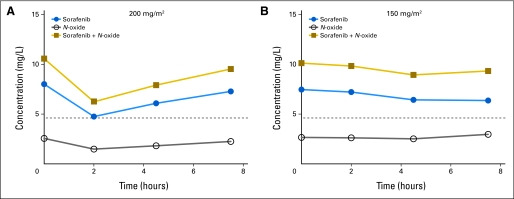
Patients and methods: Twelve patients with acute leukemia (11 with acute myeloid leukemia [AML]) received sorafenib on days 1 to 7 and then concurrently with cytarabine (1 g/m(2)) and clofarabine (stratum one: 40 mg/m(2), n = 10; stratum two [recent transplantation or fungal infection]: 20 mg/m(2), n = 2) on days 8 to 12. Sorafenib was continued until day 28 if tolerated. Two sorafenib dose levels (200 mg/m(2) and 150 mg/m(2) twice daily) were planned. Sorafenib pharmacokinetic and pharmacodynamic studies were performed on days 7 and 8.
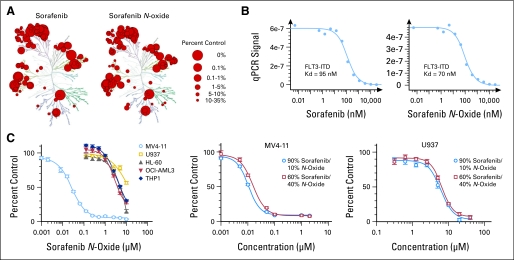
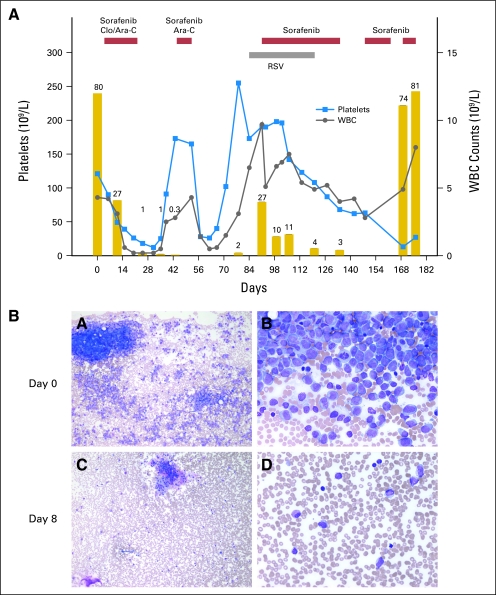
Results: At sorafenib 200 mg/m(2), two of four patients in stratum one and one of two patients in stratum two had grade 3 hand-foot skin reaction and/or rash as dose-limiting toxicities (DLTs). No DLTs were observed in six patients in stratum one at sorafenib 150 mg/m(2). Sorafenib inhibited the phosphorylation of AKT, S6 ribosomal protein, and 4E-BP1 in leukemia cells. The rate of sorafenib conversion to its metabolite sorafenib N-oxide was high (mean, 33%; range, 17% to 69%). In vitro, the N-oxide potently inhibited FLT3-internal tandem duplication (ITD; binding constant, 70 nmol/L) and the viability of five AML cell lines. On day 8, sorafenib decreased blast percentages in 10 of 12 patients (median, 66%; range, 9% to 95%). After combination chemotherapy, six patients (three FLT3-ITD and three FLT3 wild-type AML) achieved complete remission, two (both FLT3-ITD AML) had complete remission with incomplete blood count recovery, and one (FLT3 wild-type AML) had partial remission.
Conclusion: Sorafenib in combination with clofarabine and cytarabine is tolerable and shows activity in relapsed/refractory pediatric AML.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Similar articles
-
Sorafenib as monotherapy or in association with cytarabine and clofarabine for the treatment of relapsed/refractory FLT3 ITD-positive advanced acute myeloid leukemia.Clin Lymphoma Myeloma Leuk. 2014 Feb;14(1):e13-7. doi: 10.1016/j.clml.2013.08.005. Epub 2013 Oct 19. Clin Lymphoma Myeloma Leuk. 2014. PMID: 24144836 No abstract available.
-
Activity of the multikinase inhibitor sorafenib in combination with cytarabine in acute myeloid leukemia.J Natl Cancer Inst. 2011 Jun 8;103(11):893-905. doi: 10.1093/jnci/djr107. Epub 2011 Apr 12. J Natl Cancer Inst. 2011. PMID: 21487100 Free PMC article.
-
Report of a phase II study of clofarabine and cytarabine in de novo and relapsed and refractory AML patients and in selected elderly patients at high risk for anthracycline toxicity.Oncologist. 2011;16(2):197-206. doi: 10.1634/theoncologist.2010-0220. Epub 2011 Jan 27. Oncologist. 2011. PMID: 21273514 Free PMC article. Clinical Trial.
-
Hypertension and Life-Threatening Bleeding in Children with Relapsed Acute Myeloblastic Leukemia Treated with FLT3 Inhibitors.Turk J Haematol. 2015 Sep;32(3):263-6. doi: 10.4274/tjh.2014.0250. Epub 2015 Apr 27. Turk J Haematol. 2015. PMID: 25912283 Free PMC article. Review.
-
The role of Clofarabine in the treatment of adults with acute myeloid leukemia.Crit Rev Oncol Hematol. 2015 Mar;93(3):237-45. doi: 10.1016/j.critrevonc.2014.10.009. Epub 2014 Oct 22. Crit Rev Oncol Hematol. 2015. PMID: 25457773 Review.
Cited by
-
How I treat pediatric acute myeloid leukemia.Blood. 2012 Jun 21;119(25):5980-8. doi: 10.1182/blood-2012-02-392506. Epub 2012 May 7. Blood. 2012. PMID: 22566607 Free PMC article. Review.
-
Sorafenib N-Oxide Is an Inhibitor of Human Hepatic CYP3A4.AAPS J. 2019 Jan 9;21(2):15. doi: 10.1208/s12248-018-0262-1. AAPS J. 2019. PMID: 30627802
-
Use of FLT3 inhibitors in acute myeloid leukemia remission induction or salvage therapy: systematic review and meta-analysis.Cancer Manag Res. 2018 Aug 14;10:2635-2652. doi: 10.2147/CMAR.S166387. eCollection 2018. Cancer Manag Res. 2018. PMID: 30147364 Free PMC article.
-
Pediatric Acute Myeloid Leukemia-Past, Present, and Future.J Clin Med. 2022 Jan 19;11(3):504. doi: 10.3390/jcm11030504. J Clin Med. 2022. PMID: 35159956 Free PMC article. Review.
-
A phase I trial and pharmacokinetic study of sorafenib in children with refractory solid tumors or leukemias: a Children's Oncology Group Phase I Consortium report.Clin Cancer Res. 2012 Nov 1;18(21):6011-22. doi: 10.1158/1078-0432.CCR-11-3284. Epub 2012 Sep 7. Clin Cancer Res. 2012. PMID: 22962440 Free PMC article. Clinical Trial.
References
-
- Fabian MA, Biggs WH, 3rd, Treiber DK, et al. A small molecule-kinase interaction map for clinical kinase inhibitors. Nat Biotechnol. 2005;23:329–336. - PubMed
-
- Zhang W, Konopleva M, Shi YX, et al. Mutant FLT3: A direct target of sorafenib in acute myelogenous leukemia. J Natl Cancer Inst. 2008;100:184–198. - PubMed
-
- Steelman LS, Abrams SL, Whelan J, et al. Contributions of the Raf/MEK/ERK, PI3K/PTEN/Akt/mTOR and Jak/STAT pathways to leukemia. Leukemia. 2008;22:686–707. - PubMed
-
- Scholl C, Gilliland DG, Fröhling S. Deregulation of signaling pathways in acute myeloid leukemia. Semin Oncol. 2008;35:336–345. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
